
Chapter 12
Ouch! That Hurts: Traumatic Injuries and Deaths
IN THIS CHAPTER
![]() Looking at gunshot wounds
Looking at gunshot wounds
![]() Deciphering wounds made by cutting instruments
Deciphering wounds made by cutting instruments
![]() Understanding the ravages of blunt-force trauma
Understanding the ravages of blunt-force trauma
![]() Plugging into injuries caused by electricity
Plugging into injuries caused by electricity
![]() Investigating rape
Investigating rape
How is a bite like a gunshot wound? For that matter, what do walking into a door, cutting your finger, and being struck by lightning have in common? Each of these injuries is classified as trauma, which is a catchall term for just about anything that hurts or leaves a mark. Bumps and bruises resulting from your own klutziness and slipping on a banana peel rarely result in a criminal investigation. Crimes that result in trauma — physical and sexual abuse, murder, assaults, or even car crashes, for example — often do, and they can leave a wealth of information for investigators.
Unleashing the Power of Guns and Gun Evidence
Most people have seen guns only on TV or in movies. This artificial reference point gives no indication of the true power of the weapon. When properly maintained and used, guns are a great source of sport and fun, but when handled carelessly or in an unlawful manner, they can cause injury and death. And they can do it in a heartbeat. The fired gun cannot be unfired. The sudden explosive force is shocking. Even more shocking is the damage a bullet can do to a human being.
Gunshots wounds (GSWs) are a common cause of death in accidental, suicidal, and homicidal shootings. The mechanism of death depends upon the location and severity of the injury the bullet produces. For a gunshot to be immediately fatal, extensive trauma to the brain, heart, or upper spinal cord must occur. Otherwise death is slower and typically is caused by exsanguination (bleeding to death) or a secondary wound infection. The manner of death depends upon the intent of the person discharging the weapon. Death from a GSW obviously can’t be a natural death, but shootings never intended to harm anyone are likely to be deemed accidental, while intentionally inflicted lethal GSWs are either suicidal or homicidal.
Tracking those tricky bullets
Bullets are tricky and behave in all sorts of odd ways. They may strike the skull, sternum (breastbone), or rib and be deflected away from vital organs beneath. A bullet that ricochets off the skull may leave the body completely or burrow beneath the scalp and be found at some distance from the entrance wound. A bullet that enters the chest may strike the spinal column and be defected downward into the abdomen. This can make a bullet’s final resting place difficult to locate.
Bullets that cannot readily be located are visible under X-rays, which the surgeon or medical examiner (ME) uses to locate them. Long story short: Bullets are unpredictable, and the ME may have a hard time tracking their path through the victim.
Studying entry and exit wounds
Even when a bullet enters a body, leaving an entry wound, it does not necessarily come back out, or create an exit wound. More often than not, the bullet remains within the victim. When evaluating GSWs, an ME searches for and examines entry and exit wounds and tracks down any bullets retained within the victim. Although the distinction isn’t always apparent, the ME also attempts to distinguish between entry wounds and exit wounds because doing so can be critical in reconstructing a crime scene. Knowing the paths the bullets followed can implicate or exonerate suspects or help determine which bullet caused lethal injury.
 The character of a wound produced by a gunshot depends upon several factors, including
The character of a wound produced by a gunshot depends upon several factors, including
- The distance between the victim and the muzzle of the gun
- The caliber and velocity of the bullet
- The angle at which the bullet enters the body (if it does)
- Whether the bullet remains within the victim or passes completely through, exiting the body (a through-and-through gunshot wound)
The ME can estimate the distance from which a single bullet was fired by looking closely at the entry wound (see Figure 12-1):
- If the muzzle was 2 or more feet away from the victim, the entrance wound usually is a small hole, with an abrasion collar (a blue-black bruising effect in a halo around the point of entry). Some black smudging can also occur where the skin literally wipes the bullet clean of the burned gunpowder, grime, and oil residue it picks up as it passes through the barrel of the gun (see Figure 12-1a).
- If the muzzle was between 6 inches and 2 feet from the point of entry, the skin may appear tattooed or stippled. This effect is the result of tiny particles of gunpowder discharged from the muzzle embedded in the skin, in a speckled pattern around the wound (see Figure 12-1b).
- If the muzzle was less than 6 inches from the victim, the gunshot produces a hole, a more compact area of stippling, a surrounding area of charring (from the hot gases expelled through the muzzle), and a bright red hue to the wounded tissues (see Figure 12-1c).
- If the muzzle is pressed against the victim when the gun is fired, hot gases and particulate matter are driven directly into the skin, producing greater charring and ripping the skin in a star-shaped or stellate pattern (see Figure 12-1d).

Illustration by Nan Owen
FIGURE 12-1: The anatomy of a gunshot entry wound depends upon the distance between the gun muzzle and the point of entry. Wounds may have an abrasion collar (a), tattooing (b), charring (c), or a stellate pattern (d).
Exit wounds, on the other hand, typically are larger than entry wounds because the bullet lacerates (cuts or tears) the tissues as it forces its way out through the skin. The shape and size of an exit wound depend upon the size, speed, and shape of the bullet. For example, soft lead bullets are easily deformed as they enter and pass through the body, particularly if they strike any bony structures along the way. When that happens, the bullet may become severely misshapen, which, in turn, produces more extensive tissue damage that often results in a gaping, irregular exit wound.
Distinguishing entry wounds from exit wounds is not always easy for the ME, particularly when the exit wound is shored, which means clothing or some other material supports the wound. The ragged nature of most exit wounds is caused by the bullet ripping its way through the skin. However, if the victim’s skin is supported by tight clothing or the victim is against a wall or other structure, the skin is less likely to tear. The exit wound therefore will be smaller and less ragged, and it will look more like an entry wound.
Analyzing shotgun patterns
Generally speaking, a shotgun expels a group of projectiles, or shot, and not merely a single bullet, so it creates multiple entry wounds. Because a shotgun is not rifled — that is, the inside of the barrel doesn’t have grooves (see Chapter 18) — no identifying markings are found on the shot.
In a murder where the victim is shot with a shotgun, determining the distance between the muzzle and the victim can be critical to the outcome of the case. Taking a close look at the spread pattern of the shot helps make this determination. As a general rule, the shot spreads approximately an inch for every 3 feet it travels. The best way to determine the distance from which the gun was fired is to fire it, or perhaps one like it, using the same type of ammunition, from several distances until you find the distance that comes closest to matching the shot pattern found at the crime scene.
Slicing, Dicing, and Stabbing
When Janet Leigh’s character steps into the shower in Psycho, she steps right into the clutches of crazed Norman Bates, suffering a shower of stab wounds. That gruesome scene is one of the most well-known illustrations of penetrating or sharp-force injuries — injuries in which a sharp instrument, such as a knife, actually pierces the skin.
Sharp-force wounds can be divided into three general types:
- Stab wounds most often are homicidal and result from a pointed instrument like a knife or sword. Stab wounds usually are deeper than they are wide and are more likely to be distorted by the victim’s twisting and turning to fend off the attacker. By looking at the characteristics of the wound, an ME usually can determine the type of instrument that was used. Distinguishing a knife wound from one made with an ice pick or a screwdriver is usually easy, but identifying the exact weapon that caused the injury is virtually impossible. Two notable exceptions make things a lot easier:
- If the tip of the weapon’s blade breaks off and remains in the wound, the crime lab may be able to match the broken edge from the tip with that of a suspect weapon in a jigsaw puzzle fashion.
- If the victim’s blood can be DNA-matched (see Chapter 15) to blood found on the weapon, the evidence tells a powerful story.
-
Incised or cut wounds are caused when a sharp instrument is drawn across the skin. Unlike stab wounds, they have no characteristic width or depth and thus reveal little of the nature of the weapon. These wounds are rarely fatal, but when they are, they usually are suicidal or homicidal.
- Suicidal wounds typically are found on the victim’s wrists and, rarely, on the neck. Suicidal incised wounds frequently are accompanied by hesitation marks — smaller, shallower cuts created by the person gathering the courage to make the fatal cut.
- Homicidal incised wounds typically are seen on the neck. If the assailant is behind the victim, the cut usually extends from high up on one side near the ear, sweeps downward across the front of the throat, and then back up on the opposite side. The path of this sweep is left to right in a right-handed assailant and the opposite for a left-handed one. If an attacker is facing a victim, the cut usually is shorter and more horizontal.
- Defensive wounds can be incised in nature. As a victim attempts to fend off an attacker, the knife blade may slice the victim’s hands, wrists, forearms, and even feet.
- Accidental cuts typically involve the hands and rarely are fatal. Accidental cuts that involve the neck are extremely rare. Falling or flying glass fragments make up the majority of such neck wounds.
Accidental, suicidal, and homicidal incised wounds usually are in different areas of the body and show different cut patterns. Knowing these locations and patterns helps the ME reconstruct the death scene and determine the manner of death.
- Chop wounds are produced by heavy, sharp-edged implements, such as axes and meat cleavers. These wounds tend to be deep and wedge-shaped. Fractures and grooves often are seen in underlying bones. Lethal chop wounds usually are accidental or homicidal and rarely are suicidal. If an accidental blow (when chopping wood, for instance) severs a major artery in the leg, death can follow quickly from extensive blood loss unless immediate medical help is available.
When evaluating fatal penetrating injuries, the ME must make several determinations. First off, the ME must examine the corpse and locate each and every wound and then determine what types of weapons were likely used and which wounds were potentially lethal. One goal is to find out the sequence of the injuries and to estimate which one was the likely killing wound. In homicides, this determination becomes critical when more than one assailant is being investigated, because the person delivering the fatal wound faces more serious charges. Sometimes these determinations are obvious, and other times they’re not.
Next, the ME works to determine the manner of death. Stabs, cuts, and chopping wounds can be accidental, suicidal, or homicidal in nature, and the ME must make this distinction whenever possible by evaluating the nature, location, and number of wounds.
 Determining the type of blade that made the wound is next to impossible, but often the ME can measure the depth and width of the wound and occasionally can determine whether the blade was straight, curved, or serrated on one edge. The depth of the wound can be used to estimate the minimum length of the blade. The blade could be longer if incompletely thrust into the victim, but it can’t be shorter. However, if the knife was thrust deeply enough to leave a patterned abrasion that mirrors the knife’s hand guard around the wound, the ME may then be able to determine the blade’s actual length. The hand guard is the piece of metal between (usually perpendicular to) the handle and the blade that prevents the user’s hand from sliding down on to the blade. Whenever the hand guard impacts the skin with enough force, it can leave a bruise or abrasion that matches the guard in shape and size.
Determining the type of blade that made the wound is next to impossible, but often the ME can measure the depth and width of the wound and occasionally can determine whether the blade was straight, curved, or serrated on one edge. The depth of the wound can be used to estimate the minimum length of the blade. The blade could be longer if incompletely thrust into the victim, but it can’t be shorter. However, if the knife was thrust deeply enough to leave a patterned abrasion that mirrors the knife’s hand guard around the wound, the ME may then be able to determine the blade’s actual length. The hand guard is the piece of metal between (usually perpendicular to) the handle and the blade that prevents the user’s hand from sliding down on to the blade. Whenever the hand guard impacts the skin with enough force, it can leave a bruise or abrasion that matches the guard in shape and size.
Taking the Hit: Blunt-Force Trauma
If you’ve ever bumped into a table, hit your head on a cabinet, or caught a baseball with your face, you’ve experienced blunt-force trauma. Blunt-force trauma occurs whenever you make contact with a hard, dull object in a way that hurts you. It can come from an assault, a fall, an automobile accident, or a number of other situations, and the impact may scrape or bruise your skin, break your bones, or even damage your internal organs.
Scraping and abrading
Abrasions are injuries that result in the removal of the superficial layer of skin. Although most people call all abrasions scrapes, physicians and MEs refer to them in several different ways:
- Sliding abrasions occur when an object scrapes or brushes away the skin. Road rash is a common example that results when a pedestrian slides across pavement after being struck by an automobile. Rope nooses and other materials used for strangulation can cause scrape abrasions on the neck.
- Stamp abrasions occur when a blunt object strikes the skin, crushing it and leaving behind a raw area. These types of abrasions tend to be small and discreet and may reflect the general shape of the object that made them — a baseball bat, wooden board, or car bumper, for example.
- Patterned abrasions are a special type of stamp abrasion where the blunt object that strikes you leaves behind its pattern or the pattern of clothing or any other material between the object and your skin. A chain may leave abrasions that reveal the pattern of its links; the pattern of a car’s grillwork may be seen on the body of a hit-and-run victim. If the victim is wearing clothing with a coarse weave, the impact may likewise imprint the pattern of the weave on the victim’s skin.
Establishing when an abrasion occurred is difficult and rests on the usual healing patterns for such injuries. Unfortunately, the process doesn’t always move at a usual pace. Pathologists visually inspect these wounds in living and deceased victims and may take samples for microscopic examination from the latter.
The healing process can be divided into these five stages:
- Scab formation begins almost immediately but is not noticeable until after about six hours. The wound may ooze serum for the first 24 hours. Red blood cells are usually caught up in the dried red-brown serum that becomes the scab. The abraded area appears dark red, and when viewed under the microscope, reveals the presence of large numbers of specialized white blood cells called polymorphonuclear cells (PMNs).
- Cell regeneration, which is the reappearance of lost epithelial (skin) cells, begins about 36 hours after the injury but isn’t clearly visible until after about three days. Regeneration begins at the edges of the injured area.
- Cell growth and thickening progresses during the next five to nine days. The cells divide, grow in number, and continue the healing process.
- Remodeling occurs by about day 12, when the skin has thinned and taken on a slightly pale appearance.
- The skin completes its repair, and all remnants of the wound disappear, leaving a bleached-out color. Over the next few months the pigment regenerates. The skin regains its normal appearance by about day 20. Abrasions rarely leave permanent scars.
 Abrasions inflicted after death have a characteristic color and character that identify them as postmortem injuries. Because circulation has stopped, blood cells and serum don’t accumulate at the injury, so these scrapes take on a light brown, parchment-like appearance. If the abrasion occurs in an area of lividity (see Chapter 11), it may show some red discoloration, but cutting into the tissue will reveal the absence of hemorrhage (blood in the tissues).
Abrasions inflicted after death have a characteristic color and character that identify them as postmortem injuries. Because circulation has stopped, blood cells and serum don’t accumulate at the injury, so these scrapes take on a light brown, parchment-like appearance. If the abrasion occurs in an area of lividity (see Chapter 11), it may show some red discoloration, but cutting into the tissue will reveal the absence of hemorrhage (blood in the tissues).
The ME analyzes abrasions and scrapes with these general stages in mind; however, the stages can vary greatly from one person to the next and from one injury to another. The ME can only estimate the general age of an abrasion, but this information still may be helpful in supporting or refuting suspect and witness statements.
Bruising and battering
Contusions, or bruises, result from damage to small blood vessels in tissues at the site of a blunt-force trauma. These injured vessels leak blood, which imparts a blue-black color to the tissues. Blood collecting in a pocket beneath the skin is called a hematoma, or goose egg.
Not every trauma leaves a mark, and the absence of a visible contusion doesn’t necessarily mean that injury didn’t occur. Bruises can be so deep that they are not apparent on the skin’s surface. Some people, particularly children and the elderly, bruise more easily than others.
Like abrasions, contusions may reflect the object that caused them: A chain, for example, can leave behind a contusion in the shape of its link pattern, a board can leave a broad clear or uninjured area with a marginal bruise that has straight and parallel edges, and a handprint often becomes visible after a slap on the face or body.
In blunt-force injuries, internal organs also can be contused. In falls, automobile accidents, and serious attacks, the liver, spleen, muscles, and other organs and tissues can be bruised. The liver and spleen are particularly prone to such injuries, which are easily identified during an autopsy.
 Bruising a corpse, strangely enough, also is possible; however, because a contusion depends upon blood leaking from injured vessels, creating a bruise in a body through which the blood has stopped flowing isn’t easy. A sufficiently forceful blow to a corpse can damage blood vessels and cause the stagnant blood to leak into the area of impact.
Bruising a corpse, strangely enough, also is possible; however, because a contusion depends upon blood leaking from injured vessels, creating a bruise in a body through which the blood has stopped flowing isn’t easy. A sufficiently forceful blow to a corpse can damage blood vessels and cause the stagnant blood to leak into the area of impact.
When determining when, how, and why a contusion occurs, the ME considers the following factors:
-
Color: A contusion goes through a predictable color-change process as the body reabsorbs it. The color typically goes through a sequence from dark blue to a lighter blue to a greenish-yellow to a brownish-yellow, and it fades by about day 14.
Bruises change color as enzymes in the body break down the hemoglobin in the blood. Scavenger cells from the tissue, called macrophages, in conjunction with the circulatory system, then remove these remnants, and the contusion fades. - Size: If a victim suffers a contusing blow many minutes or hours before death, the resulting bruise is fairly diffuse and widespread (larger) around the area of impact. However, if the blow is struck perimortem (the period within a few minutes before or immediately after the time of death), the bruise is smaller and more clearly defined, primarily because the blood didn’t have time to seep into and spread through the tissues before death occurred.
-
Organ trauma: Sometimes no evidence of bruising shows up on the surfaces of a body that’s suspected of suffering from blunt-force trauma. Such is the case if bruising occurs deep within the tissues and muscles and if the victim doesn’t live long enough for bruising to seep to the surface. When the ME suspects this kind of bruising, a series of deep cuts into the muscles and down to the bones along the back, arms, and legs can sometimes reveal deeper contusions as well as contusions of the internal organs.
Bruises to internal organs vary according to which organ was injured, but most appear as dark, blue-black areas at the point of impact. The ME may also notice bleeding or a hematoma (a collection of clotted blood).
- Defensive wounds: When attacked with a blunt object, the victim almost always attempts to block the blows. For example, if being pummeled with a baseball bat, victims raise their arms to prevent the blows from striking their heads. The blows impact against the ulnar (little-finger) side of the victim’s forearm, wrists, and hands. Abrasions and contusions in these areas are termed defensive wounds.
- Lacerations: Lacerations from blunt-force trauma occur when skin is torn or ripped by the force of the impact and are more common in areas like the scalp, where the skin lies close to the bone. Blunt-force lacerations occur not only to the skin but also to internal organs. An avulsion is a severe laceration where a section of the skin or other tissue actually is torn away from underlying tissues or bone. Avulsions most often occur when the blow strikes the skin at a shallow angle.
Breaking bones
Fractures are breaks in bones that result from direct or indirect trauma. A simple fracture is a single break, a comminuted fracture is where the bone breaks in two or more places, and a compound fracture is one in which the bone protrudes through the skin.
When an object makes direct contact with a bone, it causes either a single-transverse fracture (one that occurs across the long axis of the bone) or a crush fracture (one that is composed of several fracture lines).
A crush fracture often produces a compression wedge (see Figure 12-2), which can indicate the direction of the blow. The wedge points in the direction of the force. Knowing the direction of the force helps the ME reconstruct the blow and perhaps even the sequence in which multiple injuries occurred. In automobile-pedestrian accidents, this type of fracture often is termed a bumper fracture, because it results from the impact of a vehicle’s bumper against the victim’s legs or arms.
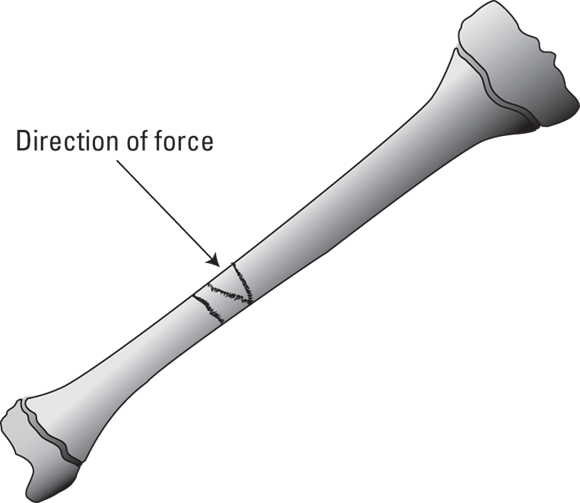
Illustration by Nan Owen
FIGURE 12-2: Crush fractures often produce a compression wedge that may indicate the direction of the force causing the injury.
Indirect fractures are not caused by a direct blow to the bone, but rather occur when an indirect force is applied to the bone with sufficient force to cause it to break. Traumatic indirect fractures are divided into four basic types (see Figure 12-3):
- Angulation fractures are simply transverse fractures that occur when a bone is bent to the point of breaking, which may occur when someone falls while his arm is trapped or held stationary. This type of injury commonly happens to children playing on playground monkey bars.
- Rotational fractures arise when a bone is twisted, causing a spiral fracture that twists down the long axis of the bone. The direction of the spiral indicates the direction of the twisting force. A child yanked or thrown by the arm can suffer such fractures.
- Compression fractures result when force is applied along the long axis of the bone, driving the bone into its end and resulting in a T- or Y-shaped break. Such fractures are sometimes seen in automobile accidents in which the victim’s knee is driven into the dashboard.
- Combination fractures are any combination of angulation, rotational, and compression fractures.

Illustration by Nan Owen
FIGURE 12-3: Indirect trauma may result in broken bones that are referred to as angulation (A), rotational (B), compression (C), or combination fractures.
Determining the age of a fracture is slightly easier than determining the age of an abrasion or contusion. Fractures heal according to the following pattern:
- Initial bleeding into the fracture site is followed by the accumulation of various types of blood cells.
- By the end of the first week, osteoblasts, which are bone-forming cells, appear.
- By the second or third week, a callus forms. This fibrous capsule-like structure surrounds the area of the fracture.
- Bone formation and the closing of the fracture within the callus take four to six weeks.
- Complete healing may take five months.
This sequence of events varies with age and from person to person. Healing is faster in the young and slower in elderly people. Determining the age of fractures is extremely important when evaluating individuals who have suffered multiple injuries over a period of time. In cases of child or elder abuse, this evidence may be critical. X-rays of severely abused individuals may show fractures that are years old as well as those that are only weeks or days old. As with bruises, whenever a physician sees a child or elderly person with fractures of varying ages, the likelihood of repeated abuse must be considered.
Getting toothy: Bite marks
The angle of your front teeth, that rough filling in your molar, and the chip you knocked out of your incisor when you crashed your bike are characteristics that make your mouth unique. Characteristics like these make dental impressions, X-rays, and dental records great tools not only for identifying bodies but also for finding criminals. Next time you eat an apple, take a look at the outline that your teeth leave in the fruit after you take a bite, and you’ll see exactly what I mean.
Bite-mark injuries occur most often in cases of murder, rape, torture, and child or spousal abuse. But bite-mark analysis deals with more than injuries inflicted upon another person. If perpetrators bite into a piece of fruit or cheese or tear a piece of tape with their teeth, they may leave valuable clues at the crime scene that police investigators or the ME can use to match the dental patterns of virtually any suspect.
Bite marks on human flesh are slightly different from the ones left in food because flesh is elastic, stretching and recoiling so details of any marks that are left are not as clear. Still, a match between the punctures and bruises left on the skin and the dental pattern of a suspect often can be made. If an individual’s teeth are damaged, chipped or are shaped in an unusual pattern, an individualizing match sometimes can result.
Because there is a lack of sufficient scientific research into bite mark analysis as well as questions about the qualifications of many examiners, this technique has recently been brought into question. Still, if the biter’s dentition shows unique features, such analysis can offer useful identifying information.
The ME often can determine whether bite marks were inflicted before death, around the time of death, or after death, by evaluating the degree of bruising. Check out the earlier “Bruising and battering” section for more about determining when bruising occurred.
After suspects are identified, molds are made of their teeth so that a model can be created. This casting then is compared with bite marks found on the victim. The lack of a match excludes the suspect, but when a match is made, it suggests, but doesn’t confirm, that the suspect is the perpetrator. More definitive follow-up testing, such as DNA matching, is required.
Bite marks on a victim should be swabbed for saliva, which can provide investigators with the perpetrator’s blood type and often a DNA profile. Chapter 15 has the details about DNA.
Moaning and groaning: My aching head
Even though most blows to the head produce injury rather than death, the head nevertheless is the most dangerous location for blunt-force trauma to occur. The brain is easily injured, and many of these injuries cause permanent damage and can lead to paralysis, blindness, loss of mental abilities, and even long-term psychiatric problems. Head and brain injuries and skull fractures most often are accidental — from falls or motor vehicle accidents, for example — but they also can be attributed to assault, homicide, or suicide.
Blunt-force head trauma can result in anything from a simple bump on the head (contusion) to concussion, which is often accompanied by a loss of consciousness, to death. To cause death, blunt-force head trauma would most likely have to cause intracranial bleeding, which occurs when an artery, vein, or many small capillaries rupture.
Bleeding into the head
The brain is covered by several membranes: The most important one is the dura mater. The space between the dura and the skull is called the epidural space, and the space between the dura and the brain is the subdural space.
Intracranial bleeds (see Figure 12-4) are of three basic types, all of which are potentially lethal:
- Epidural bleeds take place between the dura and the skull and originate in the epidural arteries, which are often torn by fractures of the skull. Automobile accidents, falls, and assaults with blunt objects can lead to such injuries.
- Subdural bleeds usually originate in the veins and occur in the space between the dura and the brain. Any blunt-force trauma to the head, even minor injuries, can lead to subdural bleeding.
- Intracerebral bleeds occur within the brain tissue itself and are most often spontaneous and caused by the rupture of abnormal or diseased arteries rather than inflicted injury.

Illustration by Nan Owen
FIGURE 12-4: Intracranial bleeds may occur within the brain itself, between the brain and the dura mater, or between the dura mater and the skull.
The skull is a rigid capsule that protects the brain. Because the skull cannot expand, intracranial bleeding causes the pressure inside the skull to rise rapidly, effectively squeezing the brain. Mounting pressure alters brain function and ultimately pushes brain material into the foramen magnum, the opening at the base of the skull where the spinal cord exits, causing the victim to lose consciousness. The part of the brainstem that controls breathing also shuts down, respiration stops, and death follows. This process can occur within minutes, hours, or days.
During an autopsy, the ME can easily determine that a blow to the head occurred by finding a contusion or abrasion of the scalp and then locating bleeding into and around the brain. The ME may then conclude that the cause of death was blunt-force injury to the brain with bleeding. The manner of death depends upon whether the blow was accidental or intentional.
Cracking the skull
Significant brain injury can occur with or without a fracture of the skull. Similarly, a fractured skull may or may not be associated with injury to the brain. Skull fractures fall into one of the following four categories (see Figure 12-5):
- Simple linear fractures occur with low-impact injuries such as falls.
- Circular fractures require more force and may result from a blow with a pipe, hammer, or similar object. The circle can be complete or incomplete.
- Stellate fractures have a star-like shape and result from localized blows that bend the skull inward and cause it to fracture along lines of stress.
- Depressed skull fractures are the result of a section of the skull being pushed inward against the brain. This fracture requires a blow of enough force to fracture the skull throughout its depth.

Illustration by Nan Owen
FIGURE 12-5: Skull fractures can be simple linear, circular, stellate, or depressed. The type of fracture may indicate the weapon or injury that caused it.
Bouncing the brain: Coup and contrecoup
During blunt-force trauma to the head, the brain may be injured at the site of impact, an injury known as a coup, or it may be injured in a slightly more complicated way.
The brain sits within the skull and is surrounded by several layers of membranes and fluid, so that it is suspended within the skull like an egg yolk inside an eggshell. It can move inside the skull, but not much, so if the skull is moving and suddenly stops, the brain may continue to move. It may move enough to actually collide with the skull, an injury referred to as a contrecoup.
In an auto accident, for example, a passenger’s head hitting the dashboard causes a coup lesion to the front of the brain, but the brain may then bounce backward and impact the back of the skull, causing a contrecoup injury.
During an autopsy, the ME may find a contusion at the site of the traumatic blow and a contusion of the brain beneath that area (coup injury) as well as contusions and bleeding in the part of the brain opposite the blow (a contrecoup injury). The latter often is more serious than the coup injury. In fact, the coup injury may not even be evident; yet, the ME nevertheless finds evidence of damage from the contrecoup injury.
A Shocking Situation: Electrocution
You may be shocked (pun intended) to discover that electricity can kill you by several different mechanisms, depending upon the voltage of the current and the duration of its application. Electricity can burn your internal organs, interfere with your heart’s rhythm, or paralyze your brain’s breathing centers, causing you to die from asphyxia (see Chapter 13). In most cases, deaths from electrical current are accidental, but the odd homicide or suicide can be chalked up to a toaster in the tub.
Wreaking havoc: Electricity’s path through your body
When electricity enters your body, it flows along the shortest path from the point of entry to the point where it’s grounded. Whether the current turns out to be deadly depends on its amperage (a measure of the amount of electric current) and the duration of contact. A low-voltage current can take several minutes to do any harm, but a high-voltage current can kill instantly.
The greatest danger from low-voltage shocks is their effect on the heart. A normal heartbeat is caused by a rhythmic pulse of electrical current that originates in the heart’s internal pacemaker and flows through the heart muscle. A low-voltage shock from an alternating-current (AC) electrical source — any device you plug into an outlet — can interfere with this natural rhythmic pulse and lead to deadly cardiac arrhythmias (changes in heart rhythm). Death is typically instantaneous when this occurs.
Death can result from even brief shocks if a current flows directly through the body to the ground. Fatal shocks from low-voltage AC cause only minor superficial burns. In half of the cases of low-voltage electrocution, no external damage from the current is evident.
High-voltage (1,000 to 8,000 volts) electrocutions occur in industrial settings and from the high-tension lines that carry current across the country and into neighborhoods. Direct contact with such lines is not necessary because the current can arc, or jump, several inches from the line to someone standing nearby. Any tall metallic object, such as a ladder or a crane arm, also can carry the current to the victim. Accidents like these frequently occur where cherry-pickers (mechanized lifts) are inappropriately used for tree trimming or TV cameras.
Shocks from high-voltage AC sources usually result in severe internal and external burning, even with only brief exposures. However, they are less likely to cause dangerous changes in the heart’s rhythm.
High-voltage currents are defibrillatory rather than fibrillatory, meaning that they convert an abnormal rhythm back to a normal one, rather than the other way around. During a cardiac arrest, the external shock that physicians give to the victim with those paddles you see on every hospital show is higher voltage and is intended to restore a normal rhythm where a deadly abnormal rhythm exists. Note, however, that high-voltage shocks can paralyze the respiratory center of the brain, causing death from asphyxia.
Assessing the damage
During an autopsy, the ME may uncover several signs of electrical injury. In some low- and all high-voltage deaths, the skin can be charred at the point of contact, the point of grounding, or both. In low-voltage electrocutions, charring may not occur, but the skin at the contact point is likely to be red and blistered.
An interesting phenomenon of electrocution deaths is the appearance of localized rigor mortis. The spasm of rigor mortis results when the adenosine triphosphate (ATP) in the muscles falls low after death. Electrocution causes muscular spasms that can consume the ATP and cause a more sudden onset of rigor in the affected area. For example, if someone grabs an electrical line with her right hand, the current passes down the right side of the body and out through the right foot; therefore, the right arm and leg may show signs of rigor long before the rest of the body.
The rare cases in which electrocution is used as a tool for homicide usually involve an electrical device being tossed into a tub of water in which someone is sitting. When that happens, no burns are found on the body, and if the device is removed before the body is found, the ME may not be able to determine the cause of death. These circumstances are less common than in the past, because electrical devices now are required to have ground-fault interrupters (GFIs), which turn them off whenever a spike in the current or resistance is detected.
The R Word: Dealing with Rape
The trauma caused by rape goes far beyond physical trauma inflicted during a violent act and may cause long-lasting psychological trauma. Rape is a heinous crime that, although it involves sex, is about aggression, control, and possibly humiliation.
For rape to be charged, the three things that must occur are
- Actual penetration
- The use of force
- The lack of consent
Penetration doesn’t need to be complete because only slight penetration is needed to meet the definition of rape. Force often is applied through violence, the threat of violence, or coercion.
All too often, rape is accompanied by homicide, either as part of the violent act or following it to prevent the victim from identifying the assailant. Rape often is part of the act of homicide committed by a serial killer, particularly where sexually sadistic types are the perpetrators. In such cases, rape almost always is part of the killer’s fantasy or part of the killer’s need to humiliate the victim.
Conducting a rape exam
Completing a rape examination of a surviving rape victim as soon after the act as possible is critical. Unfortunately, because the act often is so devastating, the victim may wait days, if not months or even years, before reporting it. On the surface, this may seem to be odd behavior for an assault victim, but rape is nothing at all like a punch in the face. It carries with it an array of emotions and social baggage that no other crime comes close to rivaling. Victims often feel ashamed, even guilty, and want to avoid the inappropriate but real feelings of social stigmatization. Remnants of Puritanical thinking and a court system that all too often puts the victim “on trial” also play roles in propagating these feelings.
The victim should be examined by a medical doctor with experience in conducting rape examinations or a specially trained nurse practitioner. Whenever possible, a female law enforcement officer should be present so that the evidence chain of custody can be maintained. The examination consists of the following:
-
The physician or nurse practitioner examines the victim’s entire body, including the genitalia for evidence of trauma such as bruises, abrasions, or lacerations, carefully noting and photographing each.
Note: The absence of signs of trauma or violence in no way negates or diminishes any claims that a rape has occurred.
- The victim’s hands are examined, and nail clippings and scrapings are collected. The assailant’s hair, blood, or skin tissues often are found clutched in the victim’s hand or beneath the fingernails.
- Any bite marks are photographed and swabbed for saliva, which may yield DNA evidence.
- Any stains found on the victim are likewise swabbed, because they may contain saliva or semen.
- As guided by the victim’s account of the assault, the examining physician obtains vaginal, anal, and oral swabs to check for DNA-containing materials.
- The victim’s pubic hair is combed for foreign hairs and fibers.
- Samples of any stains found on the victim’s clothing are taken, and the clothing is packaged and taken to the crime lab for further evaluation.
All evidence collected during the examination is turned over to law enforcement officials for transport to the crime lab for further study.
Even if no overt trauma is found, the examining physician looks for signs that sexual intercourse took place. Vaginal fluids are examined for evidence of semen. Tests for acid phosphatase, an enzyme found in abundant quantities in semen, and a P30 immunodiffusion test for a semen-specific glycoprotein, are conducted. Acid phosphatase can be present for up to 72 hours after intercourse. A problem arises, however, whenever the victim has had consensual sex during the two or three days prior to the assault. No method exists for differentiating whether elevated levels of acid phosphatase are remnants of the consensual act or the rape itself.
A search for spermatozoa also is undertaken. Motile sperm can be found in rape survivors for up to about 24 hours after intercourse, but they rarely survive longer than 12 hours. Nonmotile sperm can persist for two or three days. As sperm die off, they initially lose their tails, leaving behind only sperm heads, which can be found for up to seven days after intercourse. So, if the victim states that she last had consensual intercourse three days earlier, finding nonmotile sperm or sperm heads is of little help; however, the presence of motile sperm has nothing to do with that episode and therefore must be related to the rape.
Sperm survive longer in a dead body than they do in a living victim. The reason: Vaginas produce certain chemicals that destroy sperm, but this action stops when the heart stops, so sperm inside a dead body are destroyed only through decomposition. Sperm can be found for up to two weeks in a corpse.
Even if no sperm are found, intercourse cannot be ruled out. The assailant may have used a condom, had a previous vasectomy, failed to ejaculate, or he may be azoospermic. Azoospermia is a condition in which no sperm is present in the seminal fluid.
After the examination is complete, the victim’s injures are treated, and she is given medications to prevent pregnancy and treat any potential venereal diseases —- a wait-and-see attitude has no place in cases involving rape. The victim is tested for HIV immediately, and the test is repeated during the next several months. A rape counselor usually becomes involved immediately to help the victim with the psychological fallout from the assault.
Dealing with fatal assaults
In rape-homicides, many of the same examinations are conducted, except that an ME, rather than a treating physician, performs the examination.
At the lab, the ME initially examines the victim while clothed, looking for trace evidence and stains and attempting to match any defects in the clothing with injuries to the victim. Afterward, the victim’s clothing is removed, packaged, and sent to the crime lab for further processing. The ME’s attention then turns to the body, following the process outlined in the earlier “Conducting a rape exam” section, and conducting other necessary tests.