A lack of recognition of potential health risks from building materials
Emina Kristina Petrović, Victoria University of Wellington, Wellington, New Zealand
Abstract
This chapter reviews the exponential increase in the development of synthetic and petroleum-based chemicals since WWII. It argues that at the time of introduction, many new chemicals were (and are still) not tested for their impact on human health, which poses problems. It problematizes existing reliance on regulations and the top-down approach, by highlighting concerns that regulatory change is too slow. This chapter proposes a new approach to this problem, by evaluating the patterns in existing recognition of issues associated with the toxicity of building materials. It proposes a framework of three stages of recognition of associated health risks, which are discussed in the following three chapters.
Keywords
Indoor air toxicity; toxicity of building materials; stages of recognition of risks; user health; sustainable building materials
5.1 Introduction
This part of the book focuses on indoor toxicity from building materials. Although use of harmful substances in buildings, and in everyday life, is not new, in the last several decades a number of changes has intensified the need to consider indoor toxicity more carefully. In this chapter these changes are discussed under the subheadings of six distinct challenges, jointly contributing to a complex problem. This problem includes low recognition of the indoor air toxicity, increases in use of synthetic chemicals, issues of increased proportions of time spent indoors, problems with obtaining sufficient evidence to trigger change, delays in implementation, and the reliance of the construction literature on regulations. This chapter proposes that because of these challenges, issues with indoor air toxicity tend to be poorly recognized and the changes can be slow. Yet, it is essential to push against such trends if there is a desire to prevent buildings from adversely contributing to human health.
Part III proposes that as part of the sustainable consideration of materials it is essential to assess the totality of health impacts that these materials can pose on human health. What is the point in saving energy, and protecting the natural ecosystems, if the same choice happens to be damaging the health of the building users? This is especially relevant as many of the choices which are good for human health are also good for the natural ecosystems, by the simple extension that humans belong to the natural ecosystems themselves. Therefore, by carefully developing approaches which prioritize what is simultaneously good for the humans and the ecosystems, it should be possible to develop thinking able to elevate the real sustainability of material choices, and possibly also achieve energy savings.
Later sections of this chapter propose a new approach to this problem, by evaluating the patterns in existing recognition of issues associated with the toxicity of building materials. A framework of three stages of recognition of associated health risks is introduced, setting the scene for the subsequent three chapters.
5.2 The problem
5.2.1 Challenge 1: low recognition of indoor air toxicity
Discussion of the problem opens with the issues with low recognition of indoor air toxicity, as the most fundamental obstacle for more intense discussion in this area. In 1993 and 2000, two analyses of the actual causes of death in the US placed toxic agents as high as the fifth place (after smoking, poor diet and physical inactivity, alcohol consumption, and microbial agents; McGinnis and Foege, 1993; Mokdad et al., 2004). Both assessments considered all toxic exposures and estimated that 2%–3.5% of total mortality was associated with toxic agents, excluding tobacco smoke exposure (McGinnis and Foege, 1993; Mokdad et al., 2004). Other assessments suggest that the health impact related to indoor air pollution costs an estimated US$400 billion per year in the United States (Birkeland, 2008, p. 105). Much of these adverse impacts relate to complex reactions of human bodies to indoor toxicants. Globally, societies are witnessing an increase in the prevalence of modern diseases such as cancer, multiple allergy syndrome, allergies, asthma, autism, and attention deficit disorder (Thompson, 2004; Armstrong et al., 2007). Unfortunately, the totality of the implications of indoor toxicants are still unclear, which makes this a less obvious problem.
There is a relatively modest recognition of the problem because although clearly tangible, the health impacts seem modest against other health priorities. For example, the World Health Organization (WHO) assessment of the total worldwide impact of indoor air quality on human health revealed that indoor air pollution can be seen as responsible for 2.7% of the global burden of disease (WHO, 2002). Yet, indoor air pollution from the combustion of solid fuels (coal, firewood) was noted as the main component of this impact and it accounted for 1.6 million deaths and 39 million DALYs (disability-adjusted life years, which considers years of life lost due to both disability and death) (WHO, 2002). Pollution from solid fuels is recognized as one of the 10 most important worldwide threats to public health (WHO, 2007). This is more the problem in less developed countries, however, even in Europe as many as 2 million DALYs per year, or 2 million years of healthy life are lost annually due to the total calculated burden of diseases attributed to indoor air quality (Jantunen et al., 2011). Similar reports place risks from building materials and the associated indoor volatile organic compounds (VOCs), only after a number of other important factors, such as combustion particles, either from indoor solid fuel combustion or tobacco smoke, building dampness, and outdoor air pollution (Jantunen et al., 2011). Yet, respiratory issues are listed as three out of the top six causes of death in high-income countries, and many cancers are in the top 20 causes of death (WHO, 2016). It is this balance between the issues with toxicity indoors being a clearly tangible and real problem, yet not as acute as some other health concerns, which makes the problem challenging to fully grasp for many organizations and individuals. Recent research in environmental psychology suggests that such confusing and conflicting information can result in general passivity on the issue (Milfont, 2010; Gifford, 2011).
Concurrently, increases in related issues of asthma and allergic diseases have been clearly evident worldwide. The WHO estimates that 15 million DALYs are lost annually due to asthma, representing 1% of the total global disease burden and leading to 250,000 annual deaths worldwide (Balachandran et al., 2010). Similarly, it was estimated that by 1990, 20% of the population suffered from an allergic disease (Spengler and Chen, 2000). Interestingly, the first documented case of hay fever was recorded in the mid-19th century by a British physician who had to collect data for another 10 years before he found seven additional cases (Spengler and Chen, 2000). Thus, hay fever was first recognized as a health condition around the time of industrialization in the country where this process was most accelerated. In 2004, Sundell reported on multidisciplinary reviews of all scientific literature conducted in the Nordic countries and Europe, which established that the increasing incidence of asthma and allergy throughout the developed world in the past 30 years was probably due to environmental changes, as the period was not long enough for change through genetic evolution (Sundell, 2004). Sundell (2004) also pointed out that the then available scientific means could still not provide sufficient explanation for this change, which they interpreted as a general decrease in health.
Some of the worst prognoses expect that in 50 years everybody will have some form of cancer (Saunders, 2002), despite more than 90% of cancers probably being avoidable (Curwell and March, 2002). People are repeatedly informed of the wisdom of changing different facets of modern lifestyles to improve the chances of a healthy life, and some consider these educational efforts understate the role of the indoor environment (Armstrong et al., 2007). In 2002, Saunders illustrated these discouraging facts with the image of contemporary humanity acting like a frog in this story:
A frog jumps into a pot of water which is gradually being heated. As the water gets warmer, the frog adjusts its body temperature and continues to adjust to the increasing water temperature until, ultimately, the frog gets boiled alive.
(Saunders, 2002, p. 5).
Thus, in terms of impact on health, it can be said that indoor air quality presents a constant background “noise” contributing to total burden, although with relatively moderate currently quantifiable direct impact on mortality. From the perspective of the construction industry however, this is significant as it presents one of the rare areas where our choices can have a direct positive or negative impact on the health of buildings users. While it could take medical professionals longer before their focus can turn to health initiatives specifically designed to alleviate indoor toxicity problems, it is in our professional mandate to start making these changes without waiting for such interventions and especially before being forced by law (see Chapter 17). With the current changes towards a more sustainable construction, it is very important to integrate better consideration of the health of inhabitants as part of these changes. While we are developing processes for assessing the impact construction has on the natural environment, it is also paramount to consider the implications on human health as much if not more. Only health-neutral or even health-improving construction activities will be truly sustainable both for human life and the natural environment.
5.2.2 Challenge 2: rise of synthetic chemicals
The issue of indoor air toxicity is reasonably new compared to a long history of human involvement with building, thus there could be inherited preconceptions within the profession based on past situations which underestimate the relevance of these issues. However, because of accelerated changes in the production of building materials since WWII, it is essential to reconsider such views (Saunders, 2002). The total production of synthetic chemicals, made artificially by chemical reaction, has increased more than 10-fold: from less than 10 million metric tons in 1945 to over 110 million tons by the early 2000s (Baker-Laporte et al., 2008, p. 272). This trend has impacted many aspects of human life and the natural environment, one strand of which is chemicals used in building and furnishing materials, where synthetic chemicals can be used on their own or in various mixtures with other components that could be more natural in origin. Natural substances, such as lead and asbestos, can also present health risks. However, the main increases have been in the development of petroleum-based synthetic chemicals. The accelerated increase in total exposure has resulted in previously unprecedented problems.
The majority of products that present risk to human health have been developed relatively recently, particularly since the second half of the 19th century, and with great diversification since WWII. Around 2000, it was estimated there were more than four million registered human-made chemicals in the world with 60,000–80,000 in common use, and 1000 being added every year (Pearson, 1998, p. 61; Saunders, 2002, p. 9; Thompson, 2004, pp. 14–15). It is estimated that fewer than 2% of these synthetic chemicals have been tested for their effects on human health and more than 70% have not been tested at all (Snyder in Saunders, 2002, p. 9). It is also suggested that insufficient information exists for health assessments of 95% of chemicals used in construction products (Pacheco-Torgal, 2012). However, development of synthetic chemicals is still accelerating, with the suggestion in 2011 that “more new materials have been developed in the last 20 years than in the rest of history combined,” and these newly developed materials present about half of the materials in current use (Schörpfer, 2011, p. 19; Brownell, 2006, p 6). In addition, there is a lack of information and research on the additive and synergistic effects of combinations of chemicals (Armstrong et al., 2007, p. 61).
As a result, many new chemicals appeared in buildings after WWII and together with the tightening of building envelope in response to energy conservation needs, poorer health outcomes and indoor air quality problems were soon observed (Andersen and Gyntelberg, 2011; IBN, 2011). In the early 1980s, this culminated with the recognition of sick building syndrome (Andersen and Gyntelberg, 2011; Rostron, 1997). Although building and furnishing materials are not unique in their negative contribution to indoor air quality and health, they are recognized as important contributors in this area (Andersen and Gyntelberg, 2011; Clausen et al., 2011). Since the 1970s, the increasing air-tightness of buildings, leading to insufficient air exchange, has led to the build-up of indoor toxicants (Clausen et al., 2011, p. 221; Sundell et al., 2011). Consequently, research on indoor air quality and the impact of building and furnishing materials on human health has developed steadily since WWII, being especially proactive in the last 20–30 years (Clausen et al., 2011). Unfortunately, research is not considered to be keeping up with the need for new knowledge in this area (Clausen et al., 2011, pp. 225–226), with concerns that control of conditions in domestic spaces is even harder to achieve (Howden-Chapman and Carroll, 2004).
5.2.3 Challenge 3: indoors society
Indoor air quality is additionally important because of the increased recognition that most people spend between 80% and 93% of their time indoors (Liu and Little, 2012; Guieysse et al., 2008). In 2011, Delgado-Saborit et al. (2011) studied the time 100 British subjects spent in different environments and confirmed that 87%–91% was indoors. Another study claimed nearly 25% of US residents are affected by poor indoor air quality either at work or home (Guieysse et al., 2008). This differentiation between workplace and home is significant, because Delgado-Saborit et al. (2011) found on average for their participants that 62% of their time indoors was at home, 16% at work, 12% in other indoor environments, and 5%–7% commuting, with the average time outdoors ranging between 2% and 5%. These figures translate to an average of 14–15 hours/day at home and only 30–75 minutes/day outdoors. These proportions signal that indoor air quality at home could be an important factor in people’s health.
Some research has focused on indoor air in relation to children’s health (Phipps, 2008; Howden-Chapman et al., 2008; Thompson, 2004). Toxicology studies recognize that generally the body’s ability to biotransform and excrete toxins is less efficient at the extremes of life, as for young children such processes are not fully developed until 6–12 months of age, and sometimes as late as 6 years of age (Philp, 2001). Children also have higher metabolic rates, which increases their exposure (Philp, 2001), making them more vulnerable than adults. Furthermore, a number of toxic substances indoors are either found in household dust (Chapter 6 and Chapter 7: How substances get regulated against in the building industry: formaldehyde, phthalate plasticizers in polyvinyl chloride/vinyl) or tend to linger close to the floor (see Chapter 7), which can increase exposure for children. In addition, children, especially the very young, spend larger proportions of their time at home indoors (Phipps, 2008; Thompson, 2004), increasing the relevance of indoor air quality in homes.
Another significant development since the recognition of sick building syndrome has been investigations of ventilation rates, which have established a need for an increase first to 10 l/s per person and subsequently to a recommended 20 l/s per person (Wargocki et al., 2002). In 2002, a multidisciplinary overview of the literature established that outdoor air supply rates lower than 25 l/s per person in commercial and institutional buildings correlated with an increased risk of sick building syndrome and more short-term sick leave and reduced productivity (Wargocki et al., 2002; Sundell, 2004). It has also been suggested that improving the indoor environmental quality in all US office buildings could prevent sick building syndrome and reduce absences for millions of US office workers, while also improving work performance, with a potential annual economic benefit of $17–26 billion (Fisk et al., 2011). As a result, there has been much development in ventilation systems and better understanding of indoor air quality needs.
The workplace has been the primary focus of developments in ventilation and occupational health (ASHRAE Handbook, 2009). However, more recent studies are indicating indoor air quality in homes is generally poorer than in offices and other public buildings (Nielsen et al., 2013; Wolkoff and Nielsen, 2010). The focus on improving ventilation and air filtration systems still relies on removing the indoor air pollution once it happens, rather than removing the pollution sources. Spaces with poorer ventilation protocols, like dwellings, have not been addressed to the same level, despite the fact as stated above that people spend most of their time at home. Potentially, high reliance on mechanical ventilation is not a good approach for domestic environments, as it is impossible to regulate and insist on regular use of such systems. For many dwellings installation of such systems could be either technically difficult or financially impossible. Therefore, elimination or encapsulation of the source could prove a more effective strategy in domestic spaces.
5.2.4 Challenge 4: insufficient evidence to trigger change
One of the most significant challenges in this area is the reliance on regulations which tend to require solid evidence of adverse effects before any changes are made, and even then the changes can be rather slow. There is much debate on how to define what is unhealthy for humans. Richard Philp in his book Ecosystems and Human Health: toxicology and environmental hazards (2001) explains that toxicological studies have developed research methods to establish thresholds for acute toxicity of many substances. However, it is much harder to evaluate the impact from low-level exposure, especially if these are chronic exposures or ones that have a cumulative effect. Additionally, there is much development in understanding reproductive and geno-toxicity, when a substance is more damaging to reproductive organs or alters the genetic makeup of an unborn child. One of the factors that complicates many studies in this area is the fact that the human body has the ability to self-heal and contemporary medicine is still unable to explain why in some people or situations these self-healing mechanisms seem to be active or inactive (Philp, 2001). The discussion in the whole of Part III should be considered against this backdrop.
While such challenges have been known for a long time now, in recent years better understanding of more sophisticated underlying mechanisms in health issues related with inhalation have emerged providing some fairly new approaches to the problem. Studies on the relationship between genes and adverse reactions of inhaled pollution suggest that there is more than one genetic marker which makes an adverse reaction more likely, although the cataloguing of this is still in the early stages (Gaffney and Christiani, 2015). Similarly, research into vaccines against well-known cancers associated with inhaled pollution (such as asbestos) is still to arrive at any tangible conclusions (Tan et al., 2014). The researchers in such areas warn of the possibilities of genetic discrimination when employment in high-risk industries in concerned, which could lead to social injustice (Gaffney and Christiani, 2015). Thus, even the researchers involved with these efforts recommend the focus should still remain on exposure reduction, as increases in exposure still hold a reliably lineal relationship with increases in adverse reactions.
This inability of current knowledge to explain fully the health mechanisms underlying human health reactions to exposures to many toxicants, points towards an alternative position: a proportion of authors suggest “prudent avoidance” or the precautionary principle (Pearson, 1998; Saunders, 2002; Thompson, 2004). The precautionary principle was established as Principle 15 of the 1992 Rio Declaration on Environment and Development and states “where there are threats of serious or irreversible damage, lack of full scientific certainty shall not be used as a reason for postponing cost-effective measures to prevent environmental degradation” (Philp, 2001). Applied to domestic indoor spaces, the precautionary principle implies avoidance of building and furnishing materials suspected to be harmful to human health without waiting for proof of their harmfulness (Pearson, 1998; Saunders, 2002; Thompson, 2004).
In a sense, the healthiest approach would be to use only substances that are proven to be harmless. This approach would echo well with the definition of health by the WHO as the enjoyment of the highest attainable “state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” (WHO, 2014). A similar approach can be observed in some newer legislation which defines harmlessness as “proven to be safe” rather than “not proven to be harmful.” The New Zealand Psychoactive Substances Bill, which came into action in August 2013, stipulates that no substances are to be sold under this Bill until proven by the manufacturers to be safe, for example.
Advancements in new, human-made chemicals and materials are one outcome of the same processes that have produced better testing abilities, better understanding of possible risks, better medical ability to help people cope with and recover from different conditions, and generally much better regulatory controls, which at least theoretically aspire to protect society at large. The problem with contemporary regulations and legislation is that most are based on proof or solid scientific evidence, and until this exists it is often hard to make changes, therefore an alternative way of thinking about these issues is needed, and Part III of this book proposes one such approach.
5.2.5 Challenge 5: delays in implementation
An additional problem is that even when the need for change is clear, implementation could be quite slow. For example, although the late 1970s or early 1980s are generally seen as the time when lead was banned, its use continued past this point, and this played out differently in different industries. Because lead was historically used in water supply pipes, the regulations of the threshold for lead in drinking water were only gradually reduced, from 300 µg/L in the 1970s, to 50 µg/L in the 1980s, 25 µg/L in the 1990s, and just 10 µg/L in 2013 (Pacheco-Torgal, 2012). This gradual and consecutive set of reductions reflected the high cost of total replacement of lead pipework, which was estimated to cost in Europe around 200,000 million euros (Pacheco-Torgal, 2012). Similarly, only in 2015 was lead completely phased out as an additive to polyvinyl chloride (PVC) (Zhang et al., 2015). Similar delays are occurring in many similarly needed changes.
Part of the issue influencing delays is the great financial implications such changes would have for certain industries. A good example of this is the two articles on vinyl published in the same issue of the Indoor Air journal in 2013. Carlstedt et al. (2013) asserted that the use of soft PVC as flooring material may increase the human uptake of phthalates in infants. Published in the same issue was an article by Blakey et al. (2013) (all authors are employed in the vinyl industry) which challenged the result based on a small number of procedural imperfections this research had. Because any early work is likely to suffer from procedural imperfections, this type of swift rebuttal financially supported by the industry in question clearly presents a tangible challenge to knowledge development. Similar discussions between researchers financed by the asbestos industry and those asserting the need to recognize the health issues with the use of the material are still facing the negotiations of reparation costs for past asbestos workers (Landrigan, 2016). The costs and financial loss appear to figure strongly in resistance to and delays in implementation of change.
Finally, many existing changes rely on regulations to influence removal from the market of products containing harmful substances. The assumption appears to be that through such intervention the change will filter down to all situations. The experiences with lead and asbestos indicate that such an approach deals poorly with existing or built-in materials.
5.2.6 Challenge 6: issues in construction literature
The lack of clarity and conclusions, discussed above, puts the construction literature into an extremely difficult position. The construction industry is regulated by a number of region-specific professional standards and in many ways most construction-related activities could be seen as either related to implementation of such standards or in some cases their development. This makes it especially difficult to integrate suspicions which have not been regulated as yet. Thus, not surprisingly, construction industry literature tends to consider indoor toxicity by close following of the local regulations at the time. The problems with this approach are obvious, as the delays are magnified.
In 1986 and 2002 two different editions of Hazardous Building Materials were published (Curwell and March, 1986; Curwell et al., 2002). Although the two editions differed significantly, reflecting the changes in both regulations and materials production over the period, they jointly asserted that “[e]pidemiological research must of necessity lag behind material developments which inevitably means that the population’s health may be at risk in the intervening period” (Burgess et al., 1986, p. 3; Curwell and March, 2002, p. 1). This lag is a perpetual feature of developments in the construction industry, and the two editions of Hazardous Building Materials clearly captured the accelerated recognition of the issues associated with lead and asbestos. The 1986 edition operated within the regulatory framework of limited use of asbestos in construction and lead in paint, focusing significant effort on education about these and the need to seek for alternatives, while in the 2002 edition these concerns were only dealt with in terms of past alterations to older houses. Nevertheless, the new edition remarked “we have moved only a short distance since 1985” (Curwell and March, 2002). This perception of the slow accumulation of knowledge in this area seems reflective of the time lag between early indications of health risks with some products and the regulatory elimination of a product.
The same general features can be observed in some of the most comprehensive works on the subject. Published in the last few years are Fernando Pacheco-Torgal, Said Jalali, and Aleksandra Fucic (eds.), Toxicity of building materials (2012), Osman Attmann, Green architecture: advanced technologies and materials (2010), and John Fernandez, Material architecture: emergent materials for innovative buildings and ecological construction (2006). Such works are generally based on the recent research, but are also reflective of the regulative recommendations at the time of writing. While this can be seen as unavoidable, it tends to lead to a relatively conservative representation of the problem: only issues that are almost impossible to disprove are discussed.
The key problem here is that the subject matter is evolving fairly rapidly, making it hard for sources of this kind to keep up. However, it should be acknowledged that this area of study has been experiencing growth for many years now. In the 1950s and 1960s, such works operated as a new field in many countries and often faced not only limitations in existing knowledge, but also technical limitations, such as multiple regression analysis not being available for large data sets due to computational limitations, and no clear publishing opportunities (Andersen and Gyntelberg, 2011). With the establishment of the Indoor Air journal in 1991, a focal point for these efforts was established and in the first 20 years of its existence the journal published 843 original research or review articles (Nazaroff, 2011). These works are generally multidisciplinary and scientific in nature, and often face the challenge of providing a sufficiently scientific exploration of relatively uncharted findings. Nevertheless, some specific subdisciplines have successfully developed. For example, studies of indoor air chemistry have experienced growth at an exponential rate between 1991 and 2007, as can be seen by the number of published papers in this area, leading to the conclusion that it can be seen as a subdiscipline in its own right (Weschler, 2011). Nevertheless, there is still much need for more research on indoor air quality.
Thus, it can be concluded that although great knowledge has been developed, and some significant changes are in the pipeline, at this point the architectural or building professions generally rely on sources which reflect the regulations at the time when making decisions about material specifications. Consequently, it is difficult to anticipate likely future changes and to work to standards higher than those that are deemed acceptable by current regulations. This problem becomes even more significant when paired with subsequent regulative changes that are never retrospective as well as the frequent changes manufacturers make to individual products.
Because of these characteristics, Part III proposes a novel approach, focused on mapping out common patterns and trends, which makes it easier to anticipate the likely future progression in recognition of risks associated with certain materials.
5.3 Beyond the challenges: three stages of recognition of health risks
The ability to anticipate likely future changes is especially important in contemporary construction which is trying to respond to calls for more sustainable practices. This process itself is a change which could facilitate uptake of any number of other desirable changes, but also because much of the work in the area of sustainability tends to focus on proposing platforms of principles, such an approach could play an important role in improving awareness and practices when it comes to health issues associated with building and furnishing materials. Thus, it should not be of surprise that many sources on sustainability also briefly explain indoor air quality issues and at least provide some examples of problem substances and available alternatives. However, this is not the rule. This section develops upon the existing literature and proposes a new approach to anticipating the upcoming concerns with indoor air toxicity.
The core research question of this section of the book is whether any clear patterns can be observed in the way knowledge about risk substances is integrated into social practices. Of special interest is whether there are any significant improvements over time, and if so, what form these take.
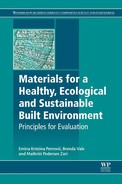
Rather than providing a detailed overview of all existing knowledge, this part uses the three key stages of progression in the recognition of risks posed by certain substances, devised to organize available information into a clear system for its interpretation, and to illustrate key patterns in the development and assimilation of new scientific knowledge. Table 5.1 summarizes the key features of each stage. Stage 1 records the early recognition of risks associated with a certain substance, Stage 2 reflects the efforts to regulate its use, often leading to a progressive decrease in allowed levels, and finally Stage 3 records the complete ban of the substance. Although for specific substances some of these stages could overlap and progress at different speeds, these stages help organize knowledge about the harmful effects of substances commonly found in building and furnishing materials, and illustrate the issues around integrating knowledge about these substances into everyday life.
This part of the book is organized by the three stages, but in a reverse order, starting with the most recognized health hazards in building and furnishing materials. Stage 3 substances, being clearly recognized as health hazards, are especially relevant for this discussion, because only they can help in evaluating the effectiveness of their elimination and how long the whole process took. Therefore, this section starts with the recognized health hazards of lead and asbestos as examples of substances in Stage 3, and these are discussed in Chapter 6.
Discussed in Chapter 7, Stage 2 substances provide good examples of the contradictions and difficulties associated with the process of starting to eliminate substances recognized as harmful. This stage could take long periods of time and include many substages. Although there is a significant qualitative difference between these substages in terms of the allowable thresholds for exposure, one reliable feature of Stage 2 is that the differentiation between these substages tends to be blurred if developments are more accelerated. This blurring is the reason they are discussed here as one stage. This blurring is especially clear for two main examples for Stage 2: formaldehyde and phthalate plasticizers. In order to provide background for Stage 2 these examples are discussed within the context of other VOCs and general issues associated with indoor air quality. The key question posed while conducting the review of Stage 2 substances is: can an acceleration of the progression from early regulations to complete ban be observed in recent years?
Finally, Chapter 8, provides a brief overview of Stage 1 substances, and evaluates the processes which surround the decisions around introducing or diversifying the use of substances that are only suspected of causing harmful effects. This is a short chapter, because for many substances this is a very quiet phase. However, it raises an important issue: is there any observable avoidance of the introduction of new chemicals into production when some concerns have been noted on the potential health impact of these? In contrast to removal, which tends to have financially adverse implications, at the point of introduction finances are invested into the application of the new substance and selecting a substance which is less likely to need subsequent elimination could be seen as financially desirable. Thus, Chapter 8, evaluates whether it is possible to observe indications of such activities becoming more common. Nanotechnology and recently developed chemicals, or those with only somewhat recognized ongoing risks are the key examples for this chapter.
Discussion of three stages of recognition from Chapters 6, 7 and 8, is followed by Chapter 9, which provides quick and indicative reviews on where many chemicals and materials sit in terms of a progression of recognition of their potential harmfulness. This highlights the importance of including systematic examination of the impacts of building materials on human health as a fundamental requirement for the development of a more sustainable built environment.
5.3.1 How hard is it to find out where the problems are?
Rather than providing a comprehensive coverage of all current issues, Part II discusses three stages of recognition of risks and uses those to illustrate the issues. The intention is to educate the reader on relevant principles and empower them to make their own similar assessments. This reflects an aspiration to provide a framework which makes it easy to move beyond practice compliant with the current regulations, and instead towards more aspirational and enduring built environments.
In order to review the impact on human health from building and furnishing materials, it was important to consider medical and other scientific primary sources. Because in many cases the product names were irrelevant for these analyses, in many cases it was important to look into specific substances or chemicals which are commonly found in well-known materials. The PubMed database was recognized as an important source when searching for an effective method of acquiring information on the established medical understanding of the health risks associated with substances used in building and furnishing materials. It is hosted by the US National Library of Medicine and comprises more than 23 million citations for biomedical literature from MEDLINE, life science journals, and online books (PubMed, 2016). Other journal articles have used PubMed as their main search tool for systematic review of literature on medical subjects. For example, Checkoway et al. (2012) searched the PubMed database of publications between 1966 and 2012 to review the association between formaldehyde exposure and lymphohematopoietic malignancies (Checkoway et al., 2012). In addition to the PubMed data base, complementary information was sourced from websites of official organizations or regulating bodies, such as WHO and the (US) Environmental Protection Agency (EPA), and some published detailed overviews, such as Toxicity of Building Materials, edited by Pacheco-Torgal, Jalali, and Fucic (2012). Thus, the chapters that follow mainly summarize the knowledge available in medical sources on subjects relevant for architectural construction materials.
5.4 Conclusion
This chapter introduced the problems associated with indoor air toxicity and proposed the use of three stages of recognition of health risks as useful in assessing the likely future regulative treatment of any specified substances. It is hard to imagine that anybody in the construction industry would intentionally set up to harm the health of either the builders or building users, and compliance with regulatory frameworks is strong in our professions. Yet, it is possible that harmful materials approved and commonly specified today could be installed in a building which would last well beyond the subsequent elimination of the same materials from everyday use. Cases of lead paint and asbestos sheets installed while still allowed are painful reminders that simple compliance with the existing regulations can lead to subsequent issues. By using the proposed stages of recognition, it is possible to anticipate likely future regulations against chemicals and make smart material choices now. Integrating such evaluations with the considerations based on Parts I and II will greatly strengthen sustainability of any built project.