
Chapter 10
Social Network Analysis and the Integration of Care
Theory and Method
Timothy R. Huerta and Roberto Dandi
Learning Objectives
- Define social network analysis and consider its utility in addressing contemporary issues in health care.
- Identify theoretical perspectives that have contributed to social network analysis as a multidisciplinary approach to the exploration of the structure of relationships.
- Examine methodological issues within social network research and assess how social network analysis offers a methodological approach to understand social structures.
- Identify distinctive features of social network research.
- Understand the levels of analysis in social network research: actors (microlevel), groups (mesolevel), and networks (macrolevel).
- Explore management implications of social network analysis.
This chapter presents the case for the application of social network analysis (SNA)—also referred to as social network theory or simply network theory—to the study of organizations generally and to health care organizations specifically. SNA helps us understand social behavior through mapping, measuring, and assessing relational data. In contrast to conventional approaches in social research, which focus on the analysis of individual-level features or variables of a person, a role, an organization, or some other entity, SNA assumes that behavior may be better explained by looking at the relations between individuals, roles, organizations, or other entities (i.e., actors) by examining the links (or ties) between nodes (Scott, 2000; Wasserman and Faust, 1994). A network then is defined as a set of interrelated nodes. As an example, an employee who is well connected within a communication network of employees may perform better than others because he or she obtains more or newer information more quickly and accurately than others do. Another type of network is the organizational chart. In this network, nodes are also employees (or organizational units), and the links among them are the authority relations, which explains who reports to whom. In SNA, nodes may be anything: employees, units, organizations, tasks, or knowledge areas. Relations may be also of any kind: formal or informal communications, alliances, or supplier-buyer contracts. Numerous dimensions characterize the relationships among nodes in relationships that allow a rich understanding of the behavior that results.
The birth of SNA can be traced to the 1930s when Jacob Moreno, the inventor of group psychotherapy, first developed sociometry as a way to map social relationships in small groups. Over the decades, SNA spread from social psychology to many disciplines, including anthropology, sociology, and organization studies (Borgatti et al., 2009). However, even if the first applications of SNA in organization science are now decades old (Tichy and Fombrun, 1979; Tichy, Tushman, and Fombrun, 1979), only recently has SNA emerged as one of the more innovative and successful fields of management and organizational research: between 2002 and 2012, 974 SNA articles were published in business and management scholarly peer-reviewed journals, beginning with just 19 in 2002, peaking at 182 in 2010, and leveling off at 132 in 2012.1
There are several explanations for this tardy success. First, only recently have relational data become increasingly available to organizational scholars, the result of the digitalization of information. Data from organizational websites, computer-mediated communications, news, and other online databases can be accessed and organized in order to extract social networks more easily now than before. Also, new data-gathering tools, such as web surveys, web “scraping,” text analysis, and data mining increasingly facilitate the extraction and organization of relational data. Second, the increasing computer power available to researchers permits the processing of larger amounts of data (and relational data) using more sophisticated (and memory-expensive) algorithms and statistical methods (such as exponential random graph models) to analyze larger social networks. Third, SNA is itself a social contagion phenomenon among researchers, partly because of its flexibility. SNA can be applied to many contexts and problems. Nodes and relations can be almost anything a researcher needs to focus on: people, units, organizations, or organizational networks themselves. Relations may be information, resource, or knowledge flows and interdependencies. As Monge and Contractor (2003) have demonstrated, SNA is a lens through which many existing organization science problems and theoretical models can be reanalyzed and reformulated.
We claim that the increased attention to SNA relates directly to the growing pressure on organizations to move from a command-and-control, silo-based, centralized, and efficiency-oriented structure (the so-called Fordist model) to a teamwork-based, flexible, decentralized, and customer-oriented structure (the so-called post-Fordist model). SNA supports this systemic and post-Fordist view of organizations. Dandi and Sammarra (2010) analyzed the text of 855 abstracts of SNA-related articles published between 1996 and 2009 in business and management research journals and found that the most central keywords of SNA discourse in management are knowledge, technology, information, group, innovation, communication, alliance, and change. Even if these concepts are very general, they can be more easily associated with a post-Fordist view of organizations than with a hierarchical and autocratic style of management. In health care, concepts like patient centeredness, interprofessional learning, teamwork, integration of different levels of care, and integration between health and social care are increasingly central to the field and fit well within an SNA framework.
In his milestone book on organizational design, Mintzberg (1978) considered health care organizations as professional bureaucracies where highly specialized professionals and nonprofessionals coordinate mostly through the standardization of knowledge. Collaboration derives from each person knowing what to do. More recently, the fragmented and interdependent nature of health care service delivery has been frequently associated by scholars with other forms of coordination occurring across boundaries: organizational (hospital/nursing home), professional (nurse/doctor), bureaucratic (Medicare/private payer), and even service line (hospital/durable medical equipment companies). Glouberman and Mintzberg (2001a 2001b), updating Mintzberg's (1978) professional bureaucracy model, argued that the standardization of capabilities is not enough for coordinating work in health care organizations. Particularly when unpredictable problems arise, only mutual adjustment between health workers can produce the required coordination.
SNA is uniquely equipped for the exploration of these relational health care issues because it is a theoretical framework through which the dynamics of relationships among multiple agents, actors, and organizations may be explored. For example, consider the US federal government's ten-year agenda, Healthy People, for a vision of “a society in which all people live long, healthy lives” (US Department of Health and Human Services, 2012). The Healthy People 2020 agenda was developed through an extensive stakeholder feedback process that included input from a consortium of over two thousand organizations; representatives from federal, state, and local governments; and public testimony. It was preceded by similar visions articulated for the 2000 and 2010 decennials. At its core, the approach of the Department of Health and Human Services (DHHS) is to involve as many stakeholders as possible in building both the vision for the future and a plan for the present that will shift the population's health from its current profile to one with improved health outcomes.
The collaborative approach of DHHS acknowledges an assumption that although organizations exist in part to perform tasks that are difficult to accomplish alone, there exists a class of problems for which no single organization is sufficient. Addressing the health of a population goes beyond the mandate of any single organization. Even in countries where medical care is controlled by national systems, such as the National Health Service in England, or provincial-level health agencies, as in Canada, efforts to influence health at the population level require multiple organizations with overlapping and even conflicting goals. Health departments, local area nonprofit entities, specialty networks like the Cardiology Network or the Transplant Network, national advocacy organizations like the American Heart Association and the American Lung Association, hub-and-spoke hospital networks, for-profit hospitals, and even police agencies all experience an overlapping of mission that makes them stakeholders in the effort to promote a healthy population. While the county department of health may provide limited direct health services, it also works with local doctors to achieve public health aims. Each of these organizations affects the bigger picture of population health and is more effective when working in concert. In short, “working in concert” may be translated into “working in a network,” which requires effective relationships among and between discrete organizations. Once there is an acknowledgment that organizations exist in a matrix of interrelationships that may be depicted as network linkages, the entire force of SNA may be invoked.
The impact of relationships in the provision of care at the macrolevel is only one of many kinds of relationships that express themselves among and within health services organizations. Relationships, both formal and informal, are foundational to the social experience of individuals and their collective efforts. Organizations simplify their expectations through focusing responsibilities into singular roles, enabling individuals to specialize in professions. Yet the act of specialization also creates barriers to engagement (Greiner and Knebel, 2003). Glouberman and Mintzberg (2001b) discuss the dynamics of professional silos in health care at length, describing the existence of entirely different realms within the hospital environment with conflicting values and perceptions that result in tensions in the relationships among professions. The discourse among academics and practitioners is therefore saturated with discussions of the need to explore relationship dynamics at the individual, organizational, community, societal, and environmental levels to better understand how structure influences both processes and outcomes. In the next section, we discuss several basic theoretical perspectives that may be used when exploring these relationships through SNA.
Social Network Analysis: A Multitheory, Multilevel Framework
Much has been written on organizational networks (see Kilduff and Tsai, 2003, and Monge and Contractor, 2003), but we draw on Astley and Van de Ven's (1983) four basic perspectives in studying organizations, which serve as a lens through which we can organize theories used in social networks: strategic choice, natural selection, collective action, and system-structural.
Strategic Choice
The concept of relationships built on strategic choice suggests that actors build relationships because they benefit directly by the tie. Theories of self-interest fall in this category and frame network behavior as organizations (actors) seeking interorganizational relationships when such network links offer a direct benefit to the organization. An economist might specify this dynamic in terms of transaction cost economics, which considers or calculates the costs associated with the creation and maintenance of any specific relationship as weighed against the benefits derived from the association. Thus, organizations seek to build relationships with those that allow them to operate more efficiently, extend their scope, increase their resources, or facilitate the long-term accomplishment of their goals.
Resource dependence theory has a significant following in the health care organization literature (Pfeffer and Salancik, 2003). Within this theory, organizations are seen as requiring resources from other organizations in the external environment, and this dynamic creates power asymmetries and interdependencies (Cook, 1977; Provan, Beyer, and Kruytbosch, 1980). This perspective places interorganizational relationships in the context of how the need for and availability of external resources influence organizational behavior. Thus, relationships are framed around gaining strategic advantage by securing access to limited resources.
In both of these cases, studies using a strategic choice perspective focus on the exchange of resources as the basis for relationships. Discussions of competitive advantage, as presented in the strategy literature, are tested against the structure of relationships. A hypothesis then may examine whether organizations that import resources (in-degree) are more successful than those that export those resources (out-degree).
Natural Selection
The term natural selection suggests the work of Darwin, which is often summarized through the phrase “survival of the fittest.” However, the theory might be better expressed as “the fittest survive.” This latter conceptualization highlights that choices influence environmental fit, and relationships may provide an adaptation advantage in that context. Organizational ecology (or population ecology) theory depicts relationships in terms of those that provide the organization the greatest chance of surviving (Baum, 1999). In these cases, organizations build relationships to improve their ability to survive environmental dynamics. Such approaches highlight variation, selection, and retention in the context of competition for scarce resources. A central assumption here is that organizations create network links to increase either their individual or collective fitness in an effort to increase the likelihood of “selection” in the Darwinian sense. An extension of this framework has been to view networks within a developmental framework. This latter work has focused on the life cycle stages of networks and the importance of building legitimacy for long-term survival (Human and Provan, 2000).
Collective Action
Theories of collective action focus on situations in which organizations create network links with each other to maximize their conjoint ability to seek or provide resources from third parties. For instance, organizations might share information to facilitate the mobilization of a community to deal with natural disasters like Hurricane Katrina. Collective action builds on the axiom that networks create a whole that is greater than the sum of its parts. For instance, in addressing complex health and human service problems, the wide sharing of knowledge and information is critical. The development of a knowledge network involves a broad set of actors functioning through a multiparty mechanism to develop a shared knowledge base that provides the ground for collaborative action (Clarke and Roome, 1999; Cummings, 2004; Tung, 2002). These interorganizational “knowledge networks” enable organizations to achieve strategic objectives by leveraging the information available from partners to a specific domain (Applegate, McFarlan, and McKenney, 1999; Premkumar and Ramamurthy, 1995).
Collective action builds on public goods theory (Olson, 1965) with the idea that individuals and organizations are motivated to join and work in networks to reap the benefits of working together. These benefits are presumably ones that could not be obtained when acting through motives of self-interest or social exchange even within a network context. Theories of collective action are useful in a broad way for explaining why organizations might form and sustain a network, and research has explored why particular network structures are formed and which structures might be most effective under particular conditions (Marwell and Oliver, 1993).
System-Structural
The fourth approach takes the concept of organization-environment and turns it on its head. Where strategic choice, collective action, and, to a lesser extent, natural selection perspectives are based on how an agent might react to an external stimulus, system-structural approaches consider relationship building as an environmental or external dynamic. For instance, in traditional schools, classrooms provide a macrolevel dynamic, which increases the likelihood that an individual might build a relationship. Individuals who share no classes in common are less likely to form relationships than those who do. Basic to understanding this perspective are four of its more common theoretical constructs: proximity, homophily, social contagion, and social persuasion.
Proximity
Proximity (or nearness) offers a powerful explanation for the maintenance of network links. Proximity has been used to explain and improve both the efficiency and effectiveness of population health delivery systems (Adams and Lin, 1998; Eisenberg and Swanson, 1996) and has also been used to optimize geographic allocations of limited health resources (Gottlieb, 1979; Kofie and Møller-Jensen, 2001; Walsh, Page, and Gesler, 1997; Wilcox, 1994). The density of social networks—that is, the degree to which an actor's ties are themselves linked with each other within the network—has been used to analyze health insurance structural forms comparatively (Grefer, 2003) and explain how health professionals' collaborations are affected by diverse social factors that include geographical proximity, social intimacy, notoriety, and education (Grimm and Chumbler, 1995). In one study, the structure of pediatricians' professional networks was found to influence how frequently physicians used clinical guidelines. Proximity was observed to be a significant influencing factor in guideline adoption, as colocated doctors were more likely to share professional norms and to have an impact on guideline use within organizations and pathologies (Dandi, Mascia, Cicchetti, and D'Alise, 2011).
Homophily
Theories of homophily are based within a theoretical framework that suggests that individuals and organizations are more likely to create links with one another if they are similar—the proverbial “birds of a feather flock together” adage (Ibarra, 1992 1993). The theoretical mechanism at play is based on a comfort zone associated with maintaining links with like-minded individuals or organizations. In his classic book The Stranger, Georg Simmel (1950) noted that individuals close to the group could not be considered strangers, but excessive distance moved people outside the group. The stranger then was someone close enough to allow interaction but far enough to create social space. By extension, social distance creates types of relationships with both opportunities and boundaries for interaction.
Other constructs are important. Academic disciplines, subject areas historically built by scholars identifying new frontiers of knowledge and applying their traditions to a problem, serve as a source of new concepts. Often these researchers seek to build critical mass as a discipline by developing a social identity that allows them to categorize the kinds of work they do—for example, biologists begat cell biologists, who begat molecular biologists, who begat genomicists. Why do genomicists identify themselves as such? Labels declare identity as a member of a focus of study that has research traditions, methods, and theorems. In this manner, disciplines grew deep, creating subdisciplines through an increasingly specialized focus (Borgatti, 2006). Furthermore, the implication of this social identity phenomenon is that the boundaries between specific disciplines and subdisciplines tend to be arbitrarily defined and subject to community standards (Wenger, 1998; Wenger and Snyder, 2000). Despite these challenges, the concept of scientific discipline is useful in that it highlights differences in the way the problem is framed and perceived by those inculcated into a specific scientific community. Discipline highlights the distinctive substantive concerns (like biological, psychological, social, and geographical phenomena), analytical levels (like cellular, cognitive, emotional, interpersonal, organizational, and community levels), concepts, measures, and methods associated with particular fields of study (Stokols et al., 2003).
Heterophily
In one study, heterophily—the tendency to interact with people having different backgrounds—was found to be prevalent within the broadly defined tobacco-harm-reduction network (Provan, Clark, and Huerta, 2008). Such findings suggest that researchers are generally more likely to interact with those in different disciplines than to collaborate with others within their discipline. Figure 10.1 illustrates the transdisciplinary network and shows the nature of the relationships. Most notably at the macrolevel, one can see the relative grouping of psychologists (squares) and chemists (triangles pointing up) among each other rather than with dissimilar others. In contrast, those in medicine are similarly connected, while at the same time, those connections are also heterophilous (Provan et al., 2008).
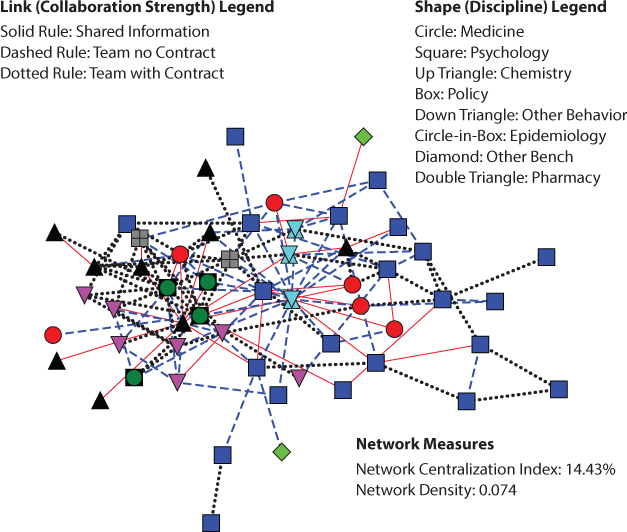
Figure 10.1 Example of a Transdisciplinary Network
Source: Adapted from the American Journal of Preventive Medicine, Vol. 35, Edition number 2, Keith G. Provan, Pamela I. Clark, and Timothy Huerta, “Transdisciplinarity among Tobacco Harm-Reduction Researchers: A Network Analytic Approach,” Pages S173-S181, 2008, with permission from Elsevier.
Social Contagion
As an organizational phenomenon, social contagion suggests that the attitudes and behaviors of organizations can be spread through relationships. The social contagion perspective considers network ties as conduits through which individual actors influence the behaviors of others, and therefore, resources available to any one person are contingent on the resources available to individuals with social proximity to them (Burt, 1987; Erickson, 1988). In this framework, greater contagion is seen among organizations that are centrally positioned in the network. This theory explores how norms are transmitted among organizations. Studies aligned with this perspective have looked at how network involvement may explain why some organizations mimic the behavior of others (Westphal, Gulati, and Shortell, 1997).
The degree of interconnectedness within networks, also named cohesion or closure, is important for predicting the level of homogeneity among actors (West et al., 1999). High closure in a social network is characterized by the frequent and diffuse exchange of information, knowledge, and other resources among individuals. High closure presumably favors the development of mutual trust and discourages opportunistic behaviors within the network. Cohesive groups are thus likely to be conducive to mechanisms of social influence and contagion.
Mechanisms of social contagion appear to be applicable to an understanding of physician behavior. A study of more than two hundred physicians in four midwestern cities in the United States revealed that the number of informal relationships between clinicians and the cohesion of their professional network affected their likelihood of prescribing new antibiotics (Coleman, Katz, and Menzel, 1966). The attitude of physicians toward new drugs included some uncertainty and ambiguity. The physicians in the study relied heavily on the opinions and judgments of their peers to better evaluate and interpret scientific-based knowledge. Therefore, information and opinions regarding new technologies and innovative behaviors spread more rapidly in high-cohesion network settings (Coleman et al., 1966).
Another approach that may explain the frequency of clinical guideline adoption is that of social persuasion (Dopson et al., 2002; Valente, 1996; Valente and Davis, 1999; Valente and Rogers, 1995). This perspective argues that certain individuals are especially relevant in light of the peculiar position they hold in the structural configuration of the professional network. These individuals, called opinion leaders, are more likely than others to influence the opinions, ideas, and behaviors of colleagues to whom they are linked. The status of physicians explains how the mechanism of social influence spreads throughout network ties. Status may derive from attributional characteristics of physicians such as tenure or affiliation to particular academic organizations or professional societies. However, it is also explained by the structural configuration of professional networks. Opinion leadership can be explored by identifying the most prestigious individuals within the professional community as a whole. Centrality indicators in SNA have been widely used for this purpose (Valente and Davis, 1999). Before we consider measurement of social networks in greater detail, we next discuss the importance of SNA in addressing contemporary issues in health care.
Role of Social Network Analysis in Health Services Delivery
The utility of a network perspective in health care is evident if we consider several particularly challenging characteristics of health care organizations and systems: specialization of knowledge, complex demand, professional autonomy, medical knowledge, and evidence-based medicine (EBM).
Specialization in Knowledge
In principle, high specialization (differentiation in the language of organizational analysts) promotes expertise and therefore quality of care, but in reality it hinders integration and continuity of care (Nicolini et al., 2007). A half-century ago, only eighteen medical specialty boards and a handful of subspecialties existed in the United States. By 2011, there were 158 specialties and subspecialties (Detsky, Gauthier, and Fuchs, 2012). Similarly, in the United Kingdom, there were nearly 100 approved medical specialties and subspecialties in 2011 (General Medical Council, 2011). In Italy, there were “only” 55 types of medical specialty schools as of 2012 according to the Ministry of University website (http://scuole-specializzazione.miur.it/) and countless subspecialties. Medical specialties can be classified as surgical versus internal medicine; age range of patients (children or elderly); organ based or technique based; and diagnostic or therapeutic. Some specialties may be multidisciplinary, such as occupational medicine, preventive medicine, disaster medicine, and gender medicine.
In other words, physicians know more and more about less and less. More important, as classic organization theory argues (Lawrence and Lorsch, 1967), as we move to differentiation through the development of specialties and subspecialties, we can expect a concomitant need for integration. Understanding the social networks that individuals construct in health care will allow interested champions to identify and analyze who knows whom or who knows who knows what, which makes the theoretical and methodological knowledge of social networks particularly useful for knowledge management (Cross et al., 2001; Dandi and Sammarra, 2009).
Complex Demand
With the aging of populations and widespread chronic diseases and comorbidities, there is today a greater need than ever before for integration of care professionals and nonprofessionals. The increasing demand for long-term care services by the elderly adds urgency to the need for better coordination between health and social care. Constraints on government and public health spending promote the creation of hub-and-spoke networks of care where economies of scale and territorial coverage are balanced. The increasing demand for quality care requires better integration between primary and acute care providers, as well as the development of information systems for the integration of patient data produced across care levels and specialties.
Shrinking Professional Autonomy
Health care organizations are made of professionals who standardize their behavior and knowledge according to their professional rules of conduct and training. As professionals, they are autonomous in clinical decisions related to specific cases. However, the diffusion of litigation, insurance costs, defensive medicine practices, the consumer movement, the increased importance of midlevel professionals, and the spread of EBM today challenge this autonomy. More and more, professionals must rely on standard procedures and interprofessional collaboration rather than their own skills.
Nature of Medical Knowledge and Difficult Knowledge Update
Heathfield and Louw (1999) have estimated that medical knowledge increases fourfold during the professional lifetime of a doctor. Doctors and health care organizations should therefore update their competencies and ensure that innovations such as new drugs, technologies, and clinical guidelines are adopted, but the superabundance of medical knowledge makes it impossible for any doctor to be thoroughly aware of all that is known about medical progress. Furthermore, even with a clear understanding of the evidence, only 10 to 20 percent of the cases that a typical doctor encounters can be handled using guidelines alone (Heathfield and Louw, 1999). For all the other cases, doctors must rely not on scientific knowledge but on their practical experience, peer collaboration, informal communication, teamwork, and the integration of different capabilities. The influence of network structure on health care professionals' clinical guideline is one of many examples in the literature that have relied on the theory and methodological approach in SNA that we explore later in the chapter.
The increasing awareness of the need to integrate people, competencies, and tasks in health care service delivery favors a network-based approach to organizational analysis and design. Organizational behavior and performance, in terms of efficiency and quality of care, are explained not only through the analysis of the characteristics of the organizations but also through the analysis of the role of their relations and coordination. Thus, SNA is an excellent approach for providing the tools and the theoretical framework that assist health care managers and policymakers in analyzing, measuring, and designing health care networks of organizations and individuals.
Evidence-Based Medicine Implementation
Quality of care is increasingly associated with the implementation of EBM and clinical guidelines in clinical practices. But a new effort must be put in place in order to link research to practice and to standardize clinical pathways across organizational and disciplinary boundaries. This is because of the so-called know-do gap, the inability to apply research results to specific patients. In other words, the incapacity of bringing the latest research results to the patient bed makes ineffective much of the effort of producing new knowledge. It has been estimated that the time for research to make its way into practice is on the order of fifteen to seventeen years (Balas and Boren, 2000). This gap may account in part for why, according to the World Health Organization, 7 million children die every year from preventable causes (Bryce et al., 2005).
Several SNA-based studies have addressed the problem of the adoption of EBM by clinical practices. An effect of the high specialization of health professionals, the overwhelming volume of new clinical research, and the tacit nature of much medical knowledge is the know-do gap. Instead of accessing explicit formal sources such as guidelines, clinicians rely on their expertise, also called mindlines, which are defined as “internalised, collectively reinforced, tacit guidelines in the head” (Gabbay and Le May, 2004, p. 1014). In this context, the term collectively reinforced refers to the manner in which clinicians develop these mindlines through “their interactions with each other and with opinion leaders, patients, and pharmaceutical representatives and by other sources of largely tacit knowledge that built on their early training and their own and their colleagues' experience” (Gabbay and Le May, 2004, p. 1014). In fact, through a process of enrichment, control, and refinement resulting from peer interaction, the individual mindline becomes a collective mindline, which is more easily implemented than guidelines.
SNA-based studies have confirmed the importance of social relationships with colleagues in the adoption of clinical guidelines (Keating et al., 2007; Salvatore, 2006). Colleagues help make sense of scientific findings that are ambiguous or not immediately applicable to the case under scrutiny (Dopson et al., 2002). A recent empirical project examining the impact of professional networks on the use of EBM guidelines among pediatricians confirmed this hypothesis (Dandi et al., 2011; Mascia, Dandi, and Di Vincenzo, 2012). By analyzing advice relationships among 120 pediatricians in seven local health authorities in Italy, these authors found that the network has a pivotal role in EBM implementation. In these cases, the authors found that networks of family pediatricians characterized by a high proportion of highly connected players is associated with a higher self-reported frequency of use of clinical guidelines. This means that the most respected pediatricians (those who are more frequently cited by the colleagues as sources of advice) are those using guidelines more often. Also, a high centrality in the network of advice relations between family pediatricians and hospital pediatricians is also associated with a higher use of EBM. In other words, pediatricians who ask more hospital colleagues for advice are more exposed to hospital EBM pathways and therefore are the most keen to use clinical guidelines.
Measurement in Social Network Research
Having considered the theoretical foundations of SNA as well as its value specific to health services research, we proceed to explore methodological issues within social network research. We begin by addressing some of the distinctive features of SNA, followed by consideration of different levels of analysis. There are three cross-cutting similarities to SNA studies, and these combine to produce an emerging discipline that is more than the technical properties used in analyzing network data.
SNA: Primarily Domain or Issue Focused
First, network research requires the explicit definition of a domain of interest. Underlying all network analysis is a theoretical framework that is used to suggest how and why actors engage with each other. That framework consists of questions about collaboration, collective action, cooperation, interaction, relationships, and trust. Also, organizations build relationships to match the dynamics of the environment in which they are embedded. Brandenburger and Nalebuff (1996) note that organizations build competitive and cooperative relationships in the same problem domain. Therefore, it is important to clearly define the scope of the issue that is to be studied. We provide two examples. The first, the Italian National Transplant Network, is an interorganizational multilevel formal network. The second explores the informal network engagement created by efforts to deal with the obesity epidemic in the United States.
The National Transplant Network is responsible for coordinating organ procurement in Italy. The network is organized in four levels. First, the National Transplant Center governs the network at a national level by fixing criteria and procedures for organ sharing, training professionals, laying down national guidelines, and controlling waiting lists through the Transplant Information System. Second, three interregional centers (NITp, AIRT, and OCST) coordinate interregional organ exchanges. Third, twenty-one regional centers govern procurement and transplants at the fourth and local level, where coordinators organize the procurement and transplant processes at hospitals. The governance of the network is therefore a complex task because there is a trade-off between the need to standardize procedures at the national level and the need to protect autonomy at a local level (Dandi et al., 2013). Also, the two main processes—procurement and transplant—involve different professionals with different competencies, aims, time spans, and rewards. Given these aims, the boundary of the network includes all local hospital coordination centers (about 280).
Weight management programs are also multileveled interventions. While many programs are aimed at the individual (such as offering nutrition and lifestyle advice), success at the population level is more likely if the individual efforts coincide with interventions at the organizational level (such as healthy food options in the workplace and at home) and at the environmental level (such as community approaches to food). A comprehensive approach to obesity then requires collaboration among a mix of individuals and organizations with varied interests, talents and skills, knowledge, and resources. Furthermore, because of the complex and multidimensional factors that influence healthy living, no one approach is likely to solve the problem either. Rather, among researchers, there is a concomitant need for a high degree of collaboration that explores the complexity of the genetic, psychosocial, and environmental aspects of the problem. In this case, the issue of obesity frames the inquiry. This is important because some organizations within the network build relationships for reasons other than weight management. The failure to do so explicitly would result in a study without boundaries and, therefore, without testable hypotheses.
Relationships as the Unit of Analysis
A second reason that SNA is more than a collection of quantitative techniques resides in a key difference between SNA and most traditional methodological approaches in social science. In most studies, the individual or organization is compared or contrasted against a panel of other individuals or organizations. Consider the case where organizations employ different strategic approaches to electronic medical records (EMR) systems. Much of the research then looks at some outcome, such as productivity, and explores systematic differences that may occur as a result of these alternative approaches. In contrast, SNA looks at the relationships that exist between organizations as the unit of analysis. One can see the difference visually.
Figure 10.2 presents an idealized case of six health care facilities and the direction of patient referrals among them. At first glance, there seems to be certain basic patterns. Hospital C, the general hospital, receives referrals from all facilities but does not refer out to all those facilities. One might record the data about the Referral status (R) between facility A and B as RAB = 1. However, because there is no reciprocal referral relationship, the status of that relationship might be recorded as RBA = 0. The relationship between any two actors in a network is often called a dyad. SNA then is a method for exploring the structural relationship among actors. The data of these relationships are generally recorded in matrix form, as illustrated in table 10.1.
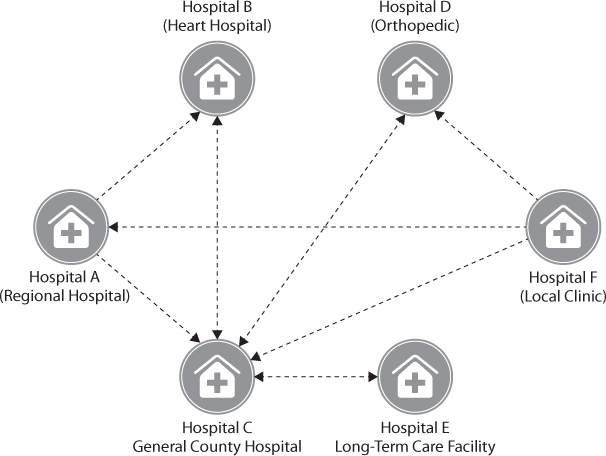
Figure 10.2 A Network of Interhospital Referrals
Table 10.1 Matrix of Relationships from Figure 10.2
| Hospital | |||||||
| A | B | C | D | E | F | ||
| Hospital | A | 0 | 1 | 1 | 0 | 0 | 0 |
| B | 0 | 0 | 1 | 0 | 0 | 0 | |
| C | 0 | 1 | 0 | 1 | 1 | 0 | |
| D | 0 | 0 | 1 | 0 | 0 | 0 | |
| E | 0 | 0 | 1 | 0 | 0 | 0 | |
| F | 1 | 0 | 1 | 1 | 0 | 0 | |
In the Italian Transplant Network case, the nodes are procurement and transplant hospitals, and relationships are organ exchanges. Organs are procured by hospitals' local procurement coordinators through a continuous monitoring of potential donors within intensive care units. The procured organ is then assigned to a patient on a regional waiting list. If no patient can be matched in a region, the interregional information system assigns the organ to another region. Transplant hospitals in the region of the receiving patient then either receive organs through an emergency shipping system or send its surgeons to the procurement hospital in order to remove it. This procedure is highly inefficient, but it is required for some types of organs because of the different surgical capacities across hospitals. Organs may be wasted if they are removed using a different surgical approach from that of the transplant surgeon who will receive the organ. Therefore, it is key for the network to minimize the distances between procurement and transplant hospitals. In this case, SNA is being used to develop an indicator for efficient organ exchanges. The average number of kilometers per organ per transplant hospital is calculated in order to measure the efficiency of the different levels of the network: transplant hospitals, regions, and interregional centers.
SNA Requires More Than Two Actors
Third, SNA requires that the domain studied include no fewer than three individuals, groups, or organizations. In most applications of SNA where primary data collection is involved, we tend to see fewer than one hundred actors, in part because of the complexity associated with achieving an 80 percent response rate when one increases the number of actors. The complexity of responding to SNA surveys is a clear stumbling block, and there are two general approaches to the establishment of the domain for a study. The first is an a priori definition based on clear external criteria. However, analysis of secondary data, especially in cases of online social dynamics, can span thousands or hundreds of thousands of individuals.
In cases of primary data collection, where actors are well known and there is a commitment to exploring some structural dynamic, SNA can be immensely powerful as a means to illustrate social dynamics. However, where the domain is not well understood, the frame can be established using the reputational or snowball sampling approach (Knoke and Kuklinski, 1982; Scott, 2000). This approach depends on researchers identifying a core sampling pool for inclusion and then engaging in an iterative process that relies on the cumulative knowledge of network members or participants about who is involved in the network. This then determines which organizations will be asked to participate and identifies the organizations that meet specific inclusion criteria in the context of each case. Reputational sampling also identifies key individuals within each organization that are most likely to be knowledgeable about the network activities and involvement of their organization. In large and diverse service organizations, it may be necessary to survey many individuals from the same organization, and in these cases, responses can be aggregated to form a single organizational response.
Actors, Cliques, and Collectives: Levels of Analysis in SNA Metrics
SNA has developed along three distinct lines, each relating to a specific level of analysis. Actor-focused theories have long dominated traditional social research and are focused on trying to explain how the position of an individual or organization (the actor) in a broader network affects either the actions or outcomes of the whole network or the other actors within the network. Group-level theories on social networks focus on groupings of dyads and larger structures—triads, and cliques and clans. And network-level theories employ many of the same ideas that actor-centric researchers use to conceptualize the totality of the network. Network-level theories focus on the structure of the whole rather than any particular part. We discuss these three approaches in turn.
Actor-Focused Metrics and Research
In organizational research, the target of actor-focused research has generally been on dyadic relations (see Gulati and Gargiulo, 1999). The dyadic approach to research tends to view the network as a collection of two-party relationships rather than as a comprehensive, multiorganizational social structure in its own right. Although a number of metrics are associated with actor-focused network analysis (Brass, 1995), five major social network measures are assigned to actors. Three of these are tied to the concept of centrality, which measures the extent to which a specific actor is positioned at the center of relationships within the network.
Degree Centrality
Degree centrality is a measure of the number of links that a specific actor has within the network structure. In a network with N actors, the highest degree centrality potentially exhibited would be N—1, insofar as an actor is not expected to link to himself. In some cases, including the example in figure 10.2, degree centrality is separated into in-degree and out-degree measures. Thus, hospital C exhibits an in-degree centrality of 5 and an out-degree centrality of 3. Actor-level calculations of degree centrality provide measures of the extent to which an organization occupies a central, as opposed to a peripheral, role in the network based on the number of ties it sends or receives from other actors.
Closeness Centrality
Closeness centrality is a measure of the extent to which an actor is close to or can easily reach all the other actors in the network (Freeman, 1979; Wasserman and Faust, 1994). It is defined as the inverse of the sum of distances to all other nodes. It should then be noted that this measure is applicable only when all actors within the network are connected in some manner, as the distance between nodes in disconnected components of a network is infinite (Wasserman and Faust, 1994). Closeness centrality is significant in the exploration of how information travels. Networks containing actors with low closeness centrality experience longer time for information to spread through the network. Actors with high closeness centrality are more likely to know what is going on throughout the totality of the network.
Betweenness Centrality
This measure is determined by calculating the extent to which an individual's position in the network lies between others and can conceptually be considered as a measure of an actor's ability to broker between two other actors in the network. In figure 10.2, hospital C demonstrates a high level of betweenness centrality because others must go through it to access resources in hospital E, a long-term care facility, and vice versa. A key use of betweenness centrality is to identify individuals who are serving in bridging roles between otherwise weakly connected parts of the network. In what Burt (1992) calls “structural holes,” individuals derive competitive advantage when they identify components of the network that would otherwise be disconnected and then position themselves as the broker between these two groups. Structural holes represent an opportunity to be a broker in the flow of information and resources through relationships, and the power to control that interaction results in a centralization of influence around those positions. A significant amount of work has looked at the role of brokerage in the literature (Braithwaite, 2010; Mascia and Cicchetti, 2011; Rangachari, 2008 2010), and in this way, betweenness centrality can offer a quantitative approach to the assessment of the role that such a position plays on organizational outcomes.
Multiplexity
Multiplexity is the extent to which two actors are linked together by more than one relationship. At a more conceptual level, the relationship between organizations is often not unidimensional but rather involves many kinds of exchanges. Hospitals share referrals, but they also share information, supplies, and governing board members; they cosponsor programs, collaborate in research efforts, and exchange employees as they move between facilities. While centrality measures speak to location within a relationship network, multiplexity addresses the depth of interactions that bind together organizations.
Relationship Strength
Relationship strength is included as a measure in that not all relationships are judged by the presence or absence of a relationship. Relationships, like all other variables, can be measured in ratio, ordinal, and nominal terms. So one factor that should also be considered is how the relationship is framed in terms of its conceptual model. There exist tools in the SNA toolbox to handle binary, categorical, and continuous data.
These measures have been used in the exploration of overall group structure, relating position to a variety of factors. For instance, a body of research has benefited from SNA approaches in the study of attitude similarities within a network. Rice and Aydin (1991) found that attitudes about new technology were similar to those with whom an actor communicated frequently, including their supervisors. Walker (1985), Galaskiewicz and Burt (1991), and Burkhardt (1994) all found that actors in structurally equivalent positions within the network evaluated their environment in similar ways.
The actor-focused research frame has been used to explore how network structural position influences attitudes; however, the term structure takes a specific meaning among network scholars. There are two general perspectives on structure in this context. When discussing structural equivalence and position within a network, Wasserman and Faust (1994) point out:
Actors occupying the same position need not be in direct, or even indirect, contact with one another. For example, nurses in different hospitals occupy the position of “nurse” by virtue of similar kinds of relationships with doctors and patients, though individual nurses may not know each other, work with the same doctors, or see the same patients. (pp. 348–349)
So if two agents exhibit identical relationship patterns, they can be found to be structurally equivalent. However, it is also possible for different actors to exhibit structural equivalence in completely isolated networks. If two organizations engage in exactly the same set of activities (out of a larger set of potential activities), they can be said to be functionally equivalent within the system because they are likely to fill similar roles. They can also be identified as interest equivalent if they share common interests.
SNA has made a significant contribution to studies of the concept of positional power proposed by French and Raven (1959), in part because SNA can quantify position. Also called “legitimate power” or “formal authority,” positional power is related to the relative position and duties of the holder of the position within an organization. Brass and Burkhardt (1992) identified a relationship between degree, closeness, and betweenness centrality in work flow, communication, and friendship networks related to power. They found that the distance to the dominant coalition and departmental centrality most strongly related to perceptions of power. This research reinforced an earlier study using longitudinal models by the same team in which they found that centrality preceded power (Burkhardt and Brass, 1990). Furthermore, they noted that early adopters of new technology gained in-degree centrality and power. Interestingly, Krackhardt (1990) reinforced the idea that knowledge is power when he found that an understanding of the network structure was associated with perceptions of power in others.
Individuals are found to leverage their networks for personal gain. Granovetter (1973 1983, 1985) has played a significant role in this research through his work on weak and strong ties. His research related relationship strength (strong versus weak ties) with differential uses. For instance, when someone is looking for information (or a job), a broad social network exhibiting weak ties can offer better quality outcomes than relying on one's closest relationships. These dynamics in fact are the basis of online social networks such as LinkedIn that seek to forge connections through multiple individuals as weak ties. Loosely connected networks are difficult to manage but provide greater accessibility to interorganizational knowledge. In contrast, strong ties allow the exchange of tacit knowledge because of a more uniform understanding (Albert, 2000; Augier and Vendelo, 1999).
Furthermore, we know that different types of networks have different needs and place distinctive demands on the network (Hansen, 2002). For example, Collinson and Gregson (2003) established that service and assistance networks, information and structuring networks, and entrepreneurship and product development represent three distinct network forms.
Mesolevel Metrics and Research
A mesolevel perspective on social networks involves a focus on groupings of dyads, for instance, triads, and their larger structures—cliques and clans. This level of analysis focuses on the existence of identifiable structures within the network. An interesting study by Ennett and Bauman (1993) explored the formation of cliques within a high school. In the study, the authors draw on B. Brown (1989) to define cliques as “interaction-based clusters of adolescents who spend more time with each other than with other adolescents and who tend to share similar attitudes and behavior” (Brown, 1989, p. 189). Thus, looking at relationships in schools, one can find structural artifacts that exist above the dyad level and would be lost by looking solely at the whole network level. Mesolevel dynamics appear when individuals create cohesive groups of relationships. Mesolevel SNA focuses on whether the presence or absence of substructure is associated with the presence of social dynamics. A study by West and colleagues (1999) found that cliques play an important role in helping to define social identity and establish a sense of belonging. In cases of multidisciplinary environments, the siloing phenomenon created by different communities of practice in health care (Glouberman and Mintzberg, 2001a 2001b) creates a significant barrier to patient care and serves as one basis for the development of barriers to relationships that manifest themselves at the mesolevel.
An example of a mesolevel substructure is a triad with a focus on relationships among groups of exactly three actors. Exploring the dynamics of interactional influence within such relationships illustrates the concept of transitivity. Transitivity pertains to relationships among three actors, which we will label A, B, and C, such that A and C are connected through B. This phenomenon, called transitive triples, is summed over all potential transitive triples and provides a mesolevel perspective on betweenness centrality.
Georg Simmel (1964) argued that dynamics within triads are not reducible to their dyadic components, and he advanced a theory based on the propensity of specific triad types to form. The sixteen forms of triads derived from his work are shown in table 10.2. SNA researchers use a common typology for the identification of specific triad connections called the M-A-N system. Let us imagine a friendship between individuals A and B and a friendship between individuals A and C. Now consider the case where A and C are in fact enemies. This dynamic is called a forbidden triad because theory suggests that the tension created by A and C in their relationship with B should result in the dissolution of either the AB or BC relationship or the reconciling of AC. According to the classic M-A-N labeling scheme, each triad is classified using a three- to four-letter code. The first three characters are numbers corresponding to the number of mutual, asymmetric, and null dyads, followed by a fourth character that further distinguishes types as either D(own), (U)p, (T)ransitive, or (C)yclic. Simmel (1964) recognized that for any network with no underlying social dynamic that influenced link creation, the distribution of each type of triad is prescribed. He argued that social dynamics pushed people to other, nonrandom arrangements. He also argued that certain forms were unstable (transient) and others stable. One can think of this in terms of the old axiom, “Any friend of yours is a friend of mine.” This work was developed into a set of theories of balance to explain these relationships. In their study of five National Tobacco Control Networks, Luke and colleagues (2010) used triad analysis to test model robustness and fit, meaning that the results were robust on varying assumption based on the empirical data gathered.
Table 10.2 Triads Classified Using M-A-N Labeling
| Specialized Link Topography | |||||
| Number of Ties in Triad | D(own) | U(p) | C(yclic) | T(ransitive) | |
| 0 |  003 |
||||
| 1 |  012 |
||||
| 2 |  102 |
 021D |
 021U |
 021C |
|
| 3 |  111D |
 111U |
 030T |
 030C |
|
| 4 |  201 |
 120D |
 120U |
 120C |
|
| 5 |  210 |
||||
| 6 |  300 |
||||
At an even broader level, sociologists identified the development of structural forms that they called cliques: a set of three or more actors who share links with every other actor in the subgroup. The definition of clique was loosened to explore less tightly formed subgroups and include k-cliques (Luce, 1950), k-clubs (Alba, 1973; Mokken, 1979), and k-plexes (Seidman and Foster, 1978). K-cliques are subgroups of nodes whose shortest paths among them are all below or equal to a value “k.” K-clubs are subgroups where all the nodes are reachable within a certain diameter “k,” and K-plexes are subgroups where each node is connected to at least n-k other nodes. With the structural changes to care associated with efforts to transform care (such as patient-centered medical homes), we can expect to see the cliques that exist because professional silos alter with service delivery practices. As better data become more readily available on relationships in health care, the exploration of relationships at the mesolevel will take an increasingly prominent role.
Network-Level Metrics and Research
Network-focused metrics draw on and use many of the same ideas and measures developed by actor-centric researchers to conceptualize the totality of the network. Rather than focusing on the role or contribution of any one agent, network measures are analogous to the average in statistics—a representation of the whole through central tendency. As a result of this macrofocus, network-level metrics are useful when making comparisons among two or more networks. They are also often reported in case studies or conceptual presentations. Although some measures are averages, others are unique conceptualizations based on properties taken from graph theory, a branch of mathematics that SNA draws heavily on. Some key network-level indicators are network centrality measures, cohesiveness, reachability, symmetry, triplet census, and transitivity.
Network Centrality Measures
These measures exist for each corresponding actor-level measure. They are often appended with the name of the scholar associated with the definition of the measures; Freeman density centrality, Freeman betweenness centrality, and Freeman closeness centrality are used to provide a macrolevel measure of a network. These metrics then focus on quantifying high-order patterns among relationships within a network. A network characterized by high-density centrality is one in which individual actors are well connected, whereas sparse density networks are loose amalgamations of relationships. The former might characterize a faculty or department, and the latter might be more indicative of an academic conference. One study that explores network centrality found that directors of nursing are more central to their networks than clinical directors of medicine to theirs, and that networks of nursing directors are more hierarchical (West et al., 1999).
- Cohesiveness. Cohesiveness, the percentage of organizations not connected to the broader community of organizations, provides a numerical representation of inclusivity. It is common for a network to have isolated actors, dyads, triads, and cliques, and a measure of cohesiveness can be used to determine whether network outcomes are associated with having all organizations connected in some manner. In a similar vein, reachability is the extent to which either direct or indirect ties link actors in the network to one another. This is generally measured as the average distance among all connected actors within a network.
- Symmetry. Symmetry is the ratio of the number of symmetric to asymmetric links (or to total number of links) in a network. The issue of symmetry is difficult to handle in SNA, in part because as scholars collect data on networks, invariably some are individuals who do not participate in the research. As a result, relationships may seem unidirectional when they are symmetric and absent when they are unidirectional. However, simultaneous work by Petrescu-Prahova and Butts (2006) and Huerta (2006) found that network measures were robust above 70 percent in the face of missing data, thereby establishing a quality guideline for empirical research in the SNA literature to require at least an 80 percent response rate.
- Triplet census and transitivity. Both are measures of subgroup dynamics. The first attends to a quantitative approach to comparing the number of various triplets that one might find if there were no patterns underlying the formation of triads in contrast to what is experienced in the data. In so doing, a researcher can test to determine if the presence of specific triplet patterns can be explained by chance and, by extension, if a phenomenon beyond chance might be at work.
The influence of the A to B to C relationship is encapsulated under the concept of transitivity. For instance, if A and B are friends, and B and C are enemies, the relationship between A and C is strained, suggesting that either B and C will resolve their relationship difficulties and move to a neutral or positive relationship, or A and C will be unable to maintain a long-term relationship as their interaction becomes either neutral or negative. So from a theoretical perspective, the influence of dyadic relationships one to other dyads (thereby forming a triplet) is associated with mesolevel theory. Interest in this area has resulted in the development of a number of software programs that explore triplets, and this area of network research has expanded to include the implication of how negative and positive dyads reinforce or challenge specific triplet formation.
Network Interventions
A major ongoing debate in management research deals with the research-practice gap in management (Shapiro, Kirkman, and Courtney, 2007). Even if management is an applied discipline, evidence shows that managers, entrepreneurs, and consultants do not read or apply management research results (Shapiro et al., 2007). There are two possible explanations for this: (1) either management research focuses on the wrong topics or produces uninteresting results, or both; or (2) management scholars fail to communicate with practitioners or convince them of the utility of their results. Because we believe that SNA is not focused on the wrong topics for health care managers, we feel it is key to improve our communication with them by showing several management implications of SNA. Here we interpret and discuss some SNA-based interventions in health care settings originally proposed by Valente (2012).
First, SNA is another lens that helps the discovery of important influencers. By calculating centrality and key player measures, SNA is able to identify the most connected (important) nodes in a network. In the pediatrician network example, informal communication such as advice relationships were not considered by local health authorities for influencing the adoption and use of clinical guidelines. A management implication is that by identifying the most connected physicians in the advice network, local health authorities may try to recruit them in order to evangelize their colleagues in the use of EBM in innovation adoption or in organizational chance acceptance.
Second, SNA shows that proximity matters. Despite new information and communication technologies, physical proximity can still matter according to several studies. Proximity may be an SNA intervention tool in two ways. First, it can be used to understand network behavior. Advice relationships in the pediatrician network are more likely to occur with colleagues of the same area. Second, given this result, if proximity matters, it can be used to reshape networks. Changing the location (building, story, office, or desk) of employees affects the likelihood of the generation of social networks (friendship, collaboration, or advice). Being able to strategically use this tool may be helpful in influencing the formation of social networks that bring value to the organization.
Third, SNA may reveal bottlenecks or redundant relations. When a network map shows that all the communications between two units pass through one person, this may mean that (1) the person is dangerously irreplaceable, (2) the person may legitimately ask for more rewards or a higher responsibility, (3) the person may leave, stranding those units left behind, or (4) the person may be overloaded and form a bottleneck for communications. All of these reasons may indicate the urgent need to redesign the network by adding more links or more nodes, or both, between the two units, thus decreasing the betweenness centrality of that person. It also may be that some parts of the organization are too connected: too many meetings and too much participation may slow down decisions, thus requiring a redesign of the network structure by reformulating responsibilities.
Fourth, SNA indicators may be linked to rewards. As in the transplant network example, the SNA-based indicator of efficiency may be used to assess transplant hospital coordinators, regional coordinators, and interregional coordinators, along with other efficiency and effectiveness measures. In the tobacco research community example, a measure of interdisciplinary coauthorship may be used to reward researchers and organizational partners of the network.
Fifth, SNA may be used for team assembly by selecting the most appropriate team members in terms of attributes (skills, tenure, discipline) and social relations (past collaboration with other team members, interdependence, friendship).
Conclusion
Networks are increasingly positioned as a mechanism through which organizations engage the external environment. Although there has been a significant ongoing discussion regarding this phenomenon among funding agencies (e.g., Alberta Innovates—Health Solutions, 2013; Birdsell and Matthias, 2003; Canadian Health Services Research Foundation, 2005; Canadian Institutes of Health Research, 2008; Michael Smith Foundation for Health Research, 2013), such entities are not waiting for research to establish the value of networks as an effective organizational form in health service delivery. Be they local health integration networks (LHINs) as established in Ontario, Canada, or the taxonomy of health systems and networks developed by Bazzoli and colleagues (1999) and updated by Dubbs and colleagues (2004), network organizing has consequences.
Choosing to use a social network frame should be informed by the hypothesis a researcher is interested in testing. While it is a fascinating perspective through which to gaze at organizations, good interorganizational network research is often quite labor intensive. The participation requirements for publication can be a significant hurdle to successful completion of such research. SNA can be used as an approach to identify the structure and meaning of relationships, explain their impact, and predict how they will affect the future of individuals, organizations, and societies (Trotter, 2000). Thus, SNA can empower network stakeholders to understand and address complex issues related to structure (the linkages within the network) and process (how the network engages its members and the resources the members have access to) and to improve network functioning through an objective and systematic process as previous research efforts demonstrate (e.g., Norman and Huerta, 2006; Provan and Milward, 2001; Provan et al., 2003 2005).
Furthermore, network-level interactions focus the research at the interorganizational level as opposed to the service delivery level. This poses a challenge in network research inasmuch as a level of analysis separates the explorations of structure between organizations and the activities of organizations with their clients. For instance, in health care, interorganizational networks have service delivery organizations as their members who are charged with providing services to clients. As such, the impact of networks on clients is second order. Therefore, using client-level experiences to assess the impact of network phenomena is methodologically challenging but can be experientially rich.
Some scholars argue that SNA is in fact not a theory at all (Salancik, 1995; Scott, 2000). Rather, they claim that the study of networks is more of an attempt to study social relationships using a particular set of analytical methods and concepts, such as those previously mentioned (e.g., centrality). In other words, they argue that there is no social network theory but that it is simply a methodological approach, called SNA, useful for exploring more traditional concepts. However, we disagree with that assessment. Instead, we describe SNA in terms of the evolution of a discipline. Just as biochemists co-opted biology and chemistry to create what is now a recognized discipline, SNA has co-opted numerous theoretical frameworks in the development of a multidisciplinary approach to the exploration of social structure. Through this chapter, we have presented how SNA explores the structure of relationships among actors from both theoretical and methodological avenues. In this sense, SNA borrows from multiple theoretical perspectives and offers the ability to assess relationships at multiple levels. In the context of health care, a field defined by complexity and driven by relationships, the importance and value of applying SNA cannot be overstated.
Key Terms
- Actors
- Cliques and clans
- Cohesion
- Dyad
- Homophily
- Network centrality
- Nodes
- Organizational networks
- Proximity
- Social network analysis
- Structure
- Symmetry
- Ties
- Transitivity