Predictions
The Future of Healthcare Innovation
What’s coming down the pike? Everyone’s fascinated by the next new thing and developing trends. The reasons are obvious, and in healthcare, the stakes are always high. Impacts felt on Wall Street and Main Street include dollars, jobs, and lives saved.
The innovator must be a patient futurist, balancing enthusiasm and realism. A key requirement is accepting failure, while working toward a goal that’s often elusive. We’re building the future of medicine in a systematic, logical fashion.
The crystal ball and magic wand can illustrate the difference between what outsiders believe we do and how those in innovation see their jobs. The crystal ball is a simple lens into the future; the magic wand is a tool for channeling special talent and expertise. While having a real-time glimpse into impending genius is a privilege, innovation isn’t a passive exercise. We’re actively influencing the attributes and availability of next-generation technologies.
Sometimes I think the process is magic, because my colleagues seem to pull off great feats with intellectual and technical aplomb. In truth, it’s expertise, multiplied by elbow grease. What would be truly magical is to involve more stakeholders, especially the industry and investment community, at the early stages of innovation in our academic medical centers (AMCs) and research universities.
The Argument for Value-Based Innovation
In Chapter 5, I described the “Value of Medical Innovation.” The perspective there was to defend the notion that innovation, on the whole, made the delivery of medical care a more expensive proposition by adding costs for the development and deployment of new diagnostic and therapeutic modalities.
In this section, a small manipulation of the words to “Value-Based Innovation” seeks to represent the new movement in creative development that now takes into account the ultimate fiscal impact and appeal of innovations from the outset of the commercialization process.
Early on when innovating orthopaedic medical devices, colleagues and I joked that we’d advance a plate or prosthetic implant by “making it out of solid gold.” Flashier, complex, and more expensive seemed innovative. It’s easy to fall in love with your own ideas, especially if they reflect some level of sophistication that sets it (or presumably, the inventor) apart. That type of thinking is being squeezed out of innovation, and rightly so. The new paradigm is to deliver products and processes that increase access, improve outcomes, and demonstrate fiscal responsibility in healthcare delivery.
Cleveland Clinic is in the vanguard of Value-Based Care, moving from volume-driven, episodic, and expensive care delivery to managing populations efficiently and effectively. Simply, value can be defined by change in clinical outcome divided by cost of care. If medicine is moving to a value basis, so should innovation. As a pioneer in mission-driven innovation, Cleveland Clinic Innovations (CCI) is logically positioned to write the next chapter in commercialization and corporate venturing, value-based innovation.
The cost of innovation can be calculated, but its net effect is practically incalculable. I’ve spent my career trying to correct the misperception that innovation is expensive—or adds expense to the medical system. You can probably track expense, but it’s impossible to compute impact. The cost of developing penicillin could be tallied, but how could you determine the payback in restoration to health and lives saved?
We developed a working description for value-based innovation: Delivering solutions for big problems affecting large populations more quickly, more efficiently, and less expensively. This is the inverse of beliefs at the beginning of my career, when expense to the system was not particularly considered. Now, fiscal responsibility shares priority with potential for positively affecting patients.
The Future of Financing Healthcare Innovation
It’s difficult to bring a promising idea from the bedside to the bank. The novel concept must demonstrate clinical and scientific merit and receive significant capital infusions at critical times. It is almost unheard of for a single source of capital to finance emerging concepts from beginning to end. Instead, the investments are syndicated—multiple funding sources must be matched to development stage, size of investment, and risk tolerance.
For mission-driven innovations, initial capital typically comes from the institutions in which the ideas originate. It can be a scramble for the innovation team to assemble sufficient initial resources from various internal sources, such as research accounts, funds earmarked for innovation, philanthropic sources, and dollars directed at the CEO’s discretion. Even in institutions lacking a well-developed innovation function, I remain impressed that backing for the best ideas usually is secured.
However, relying on institutional resources is too unpredictable and inefficient. Innovation executives must seek stable assets such as grants. The federal government has traditionally been a player, through recognized funding mechanisms such as the National Institutes of Health (NIH). Individual states are starting to play an expanded role in catalyzing innovation through grants and loans that stimulate regional economic development. Federal and state leaders recognize innovation as a worthy pursuit, along with discovery science, because it creates jobs and stimulates the tax base.
Participation of Federal and State Government in Innovation
Cleveland Clinic has benefitted from federal and state government funds. The following examples represent some of the ways government funding stimulates commercialization of our promising ideas.
![]() Ohio Third Frontier (OTF). Established in 2002 and extended through at least 2015, this $2.1 billion strategic initiative focuses on creating and sustaining a statewide innovation ecosystem. Funds support the efficient transition of great ideas from the laboratory to the marketplace. The OTF uses an established award process to identify high-performing organizations and promising technologies that will benefit from critical capital infusions. An engaged, experienced 11-member commission and 16-member advisory board guide the investments. More than 60 percent of OTF dollars are directed toward healthcare and bioscience innovation and company attraction. This includes Entrepreneurial Signature Programs (ESPs) that support biomedical technology-based commercialization.
Ohio Third Frontier (OTF). Established in 2002 and extended through at least 2015, this $2.1 billion strategic initiative focuses on creating and sustaining a statewide innovation ecosystem. Funds support the efficient transition of great ideas from the laboratory to the marketplace. The OTF uses an established award process to identify high-performing organizations and promising technologies that will benefit from critical capital infusions. An engaged, experienced 11-member commission and 16-member advisory board guide the investments. More than 60 percent of OTF dollars are directed toward healthcare and bioscience innovation and company attraction. This includes Entrepreneurial Signature Programs (ESPs) that support biomedical technology-based commercialization.
CCI has been the grateful recipient of nearly $175 million, the highest percentage of funds directed to the healthcare and bioscience community. This has allowed us to establish the Global Cardiovascular Innovation Center (GCIC), our collaborative of six Ohio-based AMCs and research universities,1 among other worthwhile projects. The GCIC has become an international leader in developing, acquiring, incubating, and commercializing technologies that improve the care of diseases and disorders of the heart and blood vessels. The GCIC is located in the offices of CCI, along with about 25 of our incubating companies.
![]() JobsOhio. This is a private, nonprofit corporation designed to lead Ohio’s job-creation efforts by singularly focusing on attracting and retaining jobs, with an emphasis on strategic industry sectors in areas of statewide and regional strength. Using a private-sector approach, JobsOhio works at the speed of business, enabling Ohio to be more nimble and flexible and thus more competitive in its economic development efforts
JobsOhio. This is a private, nonprofit corporation designed to lead Ohio’s job-creation efforts by singularly focusing on attracting and retaining jobs, with an emphasis on strategic industry sectors in areas of statewide and regional strength. Using a private-sector approach, JobsOhio works at the speed of business, enabling Ohio to be more nimble and flexible and thus more competitive in its economic development efforts
![]() NIH Centers for Accelerated Innovations (NCAI). These centers offer a one-stop shop to accelerate translation of early-stage technologies for further development by the private sector and ultimately commercialization. The National Heart, Lung, and Blood Institute dedicated $31.5 million to establish three inaugural multi-institutional centers, including the NIH Center for Accelerated Innovations at Cleveland Clinic. The NIH believes that patient care and public health can be advanced by fostering collaboration to translate basic science advancements into commercially viable products.
NIH Centers for Accelerated Innovations (NCAI). These centers offer a one-stop shop to accelerate translation of early-stage technologies for further development by the private sector and ultimately commercialization. The National Heart, Lung, and Blood Institute dedicated $31.5 million to establish three inaugural multi-institutional centers, including the NIH Center for Accelerated Innovations at Cleveland Clinic. The NIH believes that patient care and public health can be advanced by fostering collaboration to translate basic science advancements into commercially viable products.
Innovation executives must be adept at identifying and accessing governmental resources such as these. Securing capital from sources that seek returns in jobs, rather than simply in revenue, can be transformative. We foresee more federal programs being directed toward innovation and that additional states will follow the lead of Ohio.
As I project the future of innovation funding, absent thus far is how to activate the industrial sector and investment community. Careful consideration and nimble execution are required to reintroduce these funders to true early-stage innovation, as venture (and even angel) investors have largely abandoned the mission-driven, organic innovation milieu.
Can Venture Capital Be Reengaged in Mission-Driven Innovation?
Mission-driven innovators and the investment community have a symbiotic relationship that historically has defined the innovation ecosystem. We use similar financial measures to track our performance, and both seek to produce results and work together. Even the most ardent innovators take a respite from describing their technology to count how much money it has raised or the number of blue-chip investors pursuing it!
But over the past decade, adverse market forces exposed tension between those who build the engine and those who supply financial fuel to make it run. The entire issue is summarized in the frequent investor lament, heard when we seek capital for nascent technologies, “Your material is too early and too risky.”
It can be difficult to counter the argument that medical innovation is expensive, risky, and long-to-market. Investors often see only the meter running on the costs of innovation and can’t calculate the human or economic impact of new ideas. These barriers don’t deter the mission-driven innovator from pursuing solutions to help humankind, but the investor still looks for returns.
Traditional venture capital has practically disengaged from the earliest and most vulnerable evolution process of new technologies. That’s a bold statement and truly not meant to diminish, deter, or disparage the venture community. It’s simply a fact that innovation leaders must accept and for which they must plan accordingly.
The venture-capital business demonstrated considerable contraction after the dot-com boom of the early 2000s, as illustrated in Figure 10.1. While the media reports signs of a rebound, the mission-driven innovation community remains concerned.
FIGURE 10.1 Trends in Venture Capital Under Management
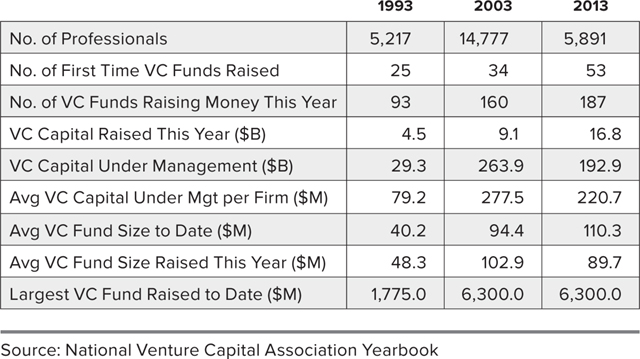
Invariably, when you drill down to what venture investors believe is investable, it’s usually companies just starting to record robust, sustainable revenues. The focus of even “smart capital” has become those few companies emerging from “the valley of death” to continue the journey toward the marketplace. Today, the early-stage definition is truly all over the map, from $2 million in revenue to north of $20 million.
I’m cautiously optimistic about the venture community. The recent surge in activity is tied largely to the more capital-efficient health information technology (HIT) startups. Big data and virtual goods and services have the promise of attracting investment closer to the starting line of development. Even therapeutics and diagnostics is demonstrating some unique models that marry the investment and commercial players.
Attracting Industry Back to Innovation with Sophisticated Financial Modeling
There’s a squeeze on funding within academic medicine resulting from the U.S. Patient Protection and Affordable Care Act (PPACA), and dwindling grant-making capabilities from historical government funders affect our colleagues in higher education. This leaves mission-driven innovation with a vital challenge: to innovate the financing model for innovation.
A mechanism must be developed to sustain the basic architecture of innovation at the AMC and research university. The first requirement is to agree on the definition of what the mission-driven innovation community actually does, how we do it, and what we aspire to accomplish.
Then we can work on reengaging our most intimate partner in innovation—the industries with whom we interface on a daily basis in a number of different venues. The way to do so is through a mechanism with two key components: ideas and capital. Exchanging ideas as currency is more straightforward to understand; we have a history of codeveloping technologies with industry partners and also welcome their intellectual properties (IP) into our innovation portfolio for further development.
But this is about attracting capital for the earliest stages of technology development. In the process of managing large amounts of IP from Cleveland Clinic and our Global Healthcare Innovations Alliance (GHIA) partners, it became increasingly clear that raising funds for each idea was exceedingly difficult and inefficient. This led to our concept of managing via a portfolio approach, each containing hundreds of gestating ideas, and spreading resources over our four CCI domains of medical devices, therapeutics and diagnostics, HIT, and delivery solutions. The portfolios have intersections such as orthopaedic medical device or cancer drugs. Some boxes are more populous than others, but there are developing opportunities in almost every intersection.
Through a stroke of serendipity, the idea of a “mutual fund” of innovation assets was coalescing about the time I was introduced to MIT Sloan School of Management finance professor Andrew Lo.
Dr. Lo is a rock-star economist, deservedly named to Time magazine’s 2012 list of The World’s 100 Most Influential People for his multidisciplinary approach to finance, using everything from statistical analysis to neuroscience to better understand markets. His theory on “adaptive markets,” in which he likens investing in innovation to messy biological systems, is genius and shows an extraordinary understanding of the entire ecosystem.
In a landmark 2012 paper in Nature Biotechnology,2 Dr. Lo and colleagues identified that large pharmaceutical concerns were distancing themselves from participation in early-stage drug development. They observed that minus 1 percent returns over the past decade had caused venture capitalists to disengage from most healthcare and bioscience startups. The resulting capital gap was diminishing U.S. innovation potential, threatening our nation’s ability to produce potentially lifesaving solutions to today’s and tomorrow’s diseases.
Dr. Lo proposed a megafund funneling up to $30 billion toward the development of new drugs, particularly those for cancer treatment. He correctly observed that the entire innovation ecosystem was ripe for something new and that securitization with a fund of unprecedented scale could unite the IP development engines of AMCs and research universities, while connecting the large pharmaceutical companies and drawing new investors to the early stages of drug creation.
In exchange for a small percentage of licensing revenue resulting from the new level of organic innovation, a win-win-win strategy would result. Academic engines would get the resources needed to continue to innovate at the most organic stages. Pharmaceutical companies would replenish their pipelines of new drugs. Dormant investors would see the spigot start to flow again, with returns tied not to a single blockbuster, but to more predictable, sustainable royalty revenues from a collection of new drugs. As mission-driven innovators, we recognized another group that would win—patients.
I was introduced to Dr. Lo by Dennis M. Kass, a member of our Innovation Advisory Board who’s become a close friend. Dennis had a distinguished public service career in the Reagan administration and a subsequent equally illustrious career in private-sector finance. Dr. Lo and Dennis not only are brilliant financial minds, their personal philosophies of integrity, benevolence, and generosity qualify them as mission-driven innovators.
Our thoughts began to clarify regarding how to bring all stakeholders in the innovation ecosystem together to ensure adequate, sustainable funding, not only for cancer drugs, but for the entire portfolio of gestating IP in our matrix.
Admittedly, the soufflé hasn’t yet risen, but the interest and enthusiasm for bringing sophisticated financial engineering concepts to the innovation ecosystem is considerable. We’re currently exploring how securitization and other financial engineering theories could revolutionize the funding of innovation in AMCs and research universities. Presently, Cleveland Clinic and MIT are engaged in building models to solve what could be the biggest threat to American creativity, the lack of adequate capital to develop it. It’s not only an opportunity for two great institutions to work together to change the face of innovation, but a responsibility to leverage our strengths on behalf of the entire community. Even venture philanthropists have expressed interest in this potential sponsorship of the innovation infrastructure that could lead to healthcare improvement across all domains.
CCI’s engagement with Dr. Lo emphasizes that innovation isn’t confined to drug discovery or medical device development. We must seek intersections of knowledge domains where innovation is most fertile, looking across all economic sectors.
This demonstrates the uniting force of mission. When the purpose is to improve and extend human life, the reason to connect is compelling and cannot simply be reduced to dollars invested or earned. However, we need to be aware of the costs and potential economic impacts, which makes innovating the way dollars flow around our ecosystem a priority for all stakeholders.
Picking the Winners: Summit and Top 10
At Cleveland Clinic, we engage in predictions at our annual Medical Innovation Summit, forecasting future healthcare advances. It provides an unrivaled perspective on evolving medical solutions and financial drivers in healthcare and bioscience. While there is an annual theme, for example, neuroscience in 2015, the summit serves as the recognized platform for interaction on all topics relevant to the world of mission-driven innovation and healthcare transformation.
The buzz that puts each annual summit at the front of business sections and news broadcasts around the country is our annual Top 10 Innovations. We share the evolving technologies that CCI leaders have identified as the most promising candidates to shape healthcare delivery over the next 12 months. Our team interviews more than 100 Cleveland Clinic and global alliance caregivers to elicit their nominations. We then employ a rigorous process to distill the opinions of Cleveland Clinic physicians and researchers, identify a roster of nominated technologies, and develop a consensus perspective of what will be the leading medical innovations for the coming year.
Nominated technologies must offer significant patient benefit in comparison to current practices, have a high probability of commercial success, and be on the market in the coming year. Adhering to our disciplined approach to every facet of medical innovation, we follow our selected technologies and keep score on how our process performed in picking the winners. It’s fascinating to see how accurate our experts prove to be.3
Ingenuity Will Create Prosperity
The political climate around the PPACA is divisive enough without considering its potential adverse effects on the medical innovation ecosystem. Some of the legislation is quite damaging, such as the 2.3 percent excise tax on medical devices manufactured in the United States or imported (Section 4191 of the Internal Revenue Code). However, there is reason to believe that ingenuity will always create prosperity, despite headwinds.
Data and popular sentiment both indicate that the pressures of Obamacare to deliver and pay for services in nontraditional ways have created pockets of opportunity in digital health, primary care, consumer-driven healthcare, and even around the concepts of risk sharing. The brightest minds have been at work for several years to determine how to identify the true barriers the legislation has erected and create fixes that improve access, quality, outcome, and cost.
To be an innovator is to be a futurist. We don’t simply peer into the unknown of tomorrow, we work to shape it. The realities of the new healthcare economy may create challenges, but if we stick to our mission and reach out for collaborators, we will advance healthcare. There is not a single solution, nor an isolated group, that could shoulder the expectation of optimizing medical innovation in the new millennium. Instead, we need input from all stakeholders and recognition from key supporters to continue to produce game-changing technologies.
We’re All Going to Be Patients
In 2012, at age 50, a gallstone lodged in my pancreas and exploded it, an extremely rare and ordinarily fatal medical problem. I spent six months hovering between life and death in Cleveland Clinic’s operating rooms and intensive care units. For the first three months of my hospitalization, the real possibility was that each day might be my last. When I turned the first corner and thought I might survive, it was a time of jubilation. But it was doubtful I would resume a normal life, and my family and I were planning for long-term care options. A couple months further into the journey, my continued improvement surprised everyone, who now believed I would eventually leave the hospital, but likely not work again. Well, in the last month of my campaign, my caregivers did such a wonderful job that I was targeting a time when I would resume my duties as Cleveland Clinic’s chief innovation officer.
What I learned over the course of this ordeal has afforded me a unique perspective on the medical system and on the importance of innovation.
![]() Make relentless forward progress. As a patient, it seemed sometimes that survival was a matter of choice, but I never gave up. The same goes for the innovator. If a project doesn’t work out, get back on the horse with fervor and enthusiasm. Whether it’s your life that’s on the line, or your ideas that could affect the lives of others, you can’t be defeatist.
Make relentless forward progress. As a patient, it seemed sometimes that survival was a matter of choice, but I never gave up. The same goes for the innovator. If a project doesn’t work out, get back on the horse with fervor and enthusiasm. Whether it’s your life that’s on the line, or your ideas that could affect the lives of others, you can’t be defeatist.
![]() You must have an advocate. It’s difficult for a patient to go it alone; you need a team of doctors, nurses, other caregivers, and loved ones. Neither can you go it alone as an inventor. You need the support of colleagues, collaborators, and your organization’s innovation leaders. Find your individual innovation champion, someone who takes an interest in you and your ideas.
You must have an advocate. It’s difficult for a patient to go it alone; you need a team of doctors, nurses, other caregivers, and loved ones. Neither can you go it alone as an inventor. You need the support of colleagues, collaborators, and your organization’s innovation leaders. Find your individual innovation champion, someone who takes an interest in you and your ideas.
![]() You should be overseen by a team. Expert caregivers working together across the lines of medical specialty translates into better patient outcomes. Similarly, a strong innovation function displays quality of leadership and level of collaboration. Seek an organization where the staff and innovation function work as a team to develop and bring ideas to market.
You should be overseen by a team. Expert caregivers working together across the lines of medical specialty translates into better patient outcomes. Similarly, a strong innovation function displays quality of leadership and level of collaboration. Seek an organization where the staff and innovation function work as a team to develop and bring ideas to market.
![]() You will need every possible source of strength. As a patient, you need the support of everyone with whom you come in contact. The power of a small gesture can be immense: a touch of the hand, sitting by your hospital bed so you can communicate at eye level. Just as I needed the gravitational pull of many to come back from the brink, innovation needs a boost from every possible sector it touches, from elected officials and philanthropists to the business and investment communities. Even patients must become more ardent advocates.
You will need every possible source of strength. As a patient, you need the support of everyone with whom you come in contact. The power of a small gesture can be immense: a touch of the hand, sitting by your hospital bed so you can communicate at eye level. Just as I needed the gravitational pull of many to come back from the brink, innovation needs a boost from every possible sector it touches, from elected officials and philanthropists to the business and investment communities. Even patients must become more ardent advocates.
![]() Life is an algorithm. As a patient, your recovery will be the sum of a thousand choices. Strive to be compliant, not complicated. Trust your caregivers and their expert consensus. Innovation is a journey with a thousand forks in the road and almost as many potholes. Prepare for more than a few side trips. Let the journey be its own reward, and put trust in the professionals handling your case. Accepting ambiguity and delay will free you to think nimbly when course correction is required.
Life is an algorithm. As a patient, your recovery will be the sum of a thousand choices. Strive to be compliant, not complicated. Trust your caregivers and their expert consensus. Innovation is a journey with a thousand forks in the road and almost as many potholes. Prepare for more than a few side trips. Let the journey be its own reward, and put trust in the professionals handling your case. Accepting ambiguity and delay will free you to think nimbly when course correction is required.
I learned before discharge that because of my 20 surgeries, I would never play golf again. I protested, “Why didn’t you tell me this was serious?” To be clear, there is nothing that can supplant the desire to return to your family after you’ve faced death, but vocational challenges and avocational pleasures are additional vital motivators.
During the months I was staring at the ceiling tiles, I tried to recall golf courses I had played to both exercise my mind and inspire myself to one day resume play. A return to Pine Valley Golf Club in New Jersey, my favorite cathedral of the game and one of its toughest physical challenges, would indicate that I had regained a normal life. I was lucky to make it back to Pine Valley the summer following my discharge.
I was granted life’s ultimate mulligan, so now I must live up to deserving it. I may have contributed modestly to the field of innovation, but I’m one of the most grateful recipients of its munificence. Innovation saved my life.
What I have learned in a lifetime that has cast me as a physician, innovator, and patient is that we play the ball where it lies. It’s challenging to script the longitudinal progression through any of these pursuits, but the chance of success is maximized by discipline, process, and collaboration. There are few guarantees in any engagement, certainly not in innovation, but one practical surety is that we will all be patients. It will be innovation that helps you or your loved ones live longer and better.
Innovation matters to each of us. Some look through the lens of the inventor, doggedly pursuing incremental or disruptive improvement in the status quo. The investor may see opportunity and return on innovation. Those of us responsible for the innovation ecosystem, at our organizations and across the world, seek to balance the requirements of stakeholders while adhering to institutional mission.
Regardless of your position in the mission-driven innovation universe, we all convene at the same point, the patient. Whether you’re a patient or an innovator, your ultimate success cannot be delivered without collaboration. It’s the responsibility of leaders in the mission-driven innovation ecosystem to be the catalyst to bring all the complex components together.
CCI is proud to be a pioneer and leading practitioner of mission-driven innovation. We’re honored to represent our institutional identity and serve our inventors. We will tirelessly continue to bring about healthcare transformation and service to our partners. I want you to join me, the Cleveland Clinic, and our Global Healthcare Innovation Alliance partners in pursuit of solutions to transform healthcare and improve lives. The ideas deserve it, the innovators deserve it, and the patients deserve it.