CHAPTER 17
Knowing Your Numbers: A Scorecard Approach to Improved Medical and Financial Outcomes
INTRODUCTION
Health literacy and chronic diseases are inextricably linked. In order to make healthy lifestyle choices to prevent chronic disease, such as exercising or limiting alcohol intake, a person must first be aware of the impact these kinds of decisions have on health, wealth, and well-being. This is not unlike the way financial literacy is associated with one's wealth, leading to decision-making that may be suboptimal. Health literacy and financial literacy are further connected because of the effect of health literacy on decisions that involve health, but have financial consequences, such as insurance and health care. This chapter proposes a short, clear, and actionable approach to overcoming health literacy barriers, thereby potentially preventing or curbing chronic disease. References to financial literacy are woven through the chapter based on the belief that a similar approach might be beneficial for improving financial decision-making and ultimately outcomes.
Health literacy is a person's ability to understand information about health and to incorporate this information into a healthy lifestyle. Key components of definitions converge, such as the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. This is linked to action through the competence to use health information and services to enhance and maintain health (Ratzan and Parker 2000) and to make appropriate health decisions and follow instructions for treatment (White 2008). Health literacy is also essential for accomplishing shared decision-making by offering the patient an active role. By comparison, a financial consumer is always required to take an active role in decision-making. Therefore, financial literacy includes a similar aspect of knowledge as a prerequisite for informed and smart financial choices.
Despite the need for comprehension, people often misunderstand medical information (Miron-Shatz et al. 2009), especially when confronted with multiple choices, as in the case of Medicare Part D, where failing to choose the most suitable medication insurance program may result in considerable financial loss (Hanoch et al. 2010). Yet, as documented in a report by the American Medical Association (White 2008), over 89 million American adults have limited health literacy skills. Given these limitations, conveying important medical and financial information in ways that are easily intelligible to the population is advisable, even at the risk of being considered simplistic. Further, while health and financial literacy belong to the individual, they can be enhanced by providing suitable materials that take into account the level of ability in the population.
Similar considerations of a population's literacy level are taken into account in the financial planning world. Financial planners and others use simple tools to assess financial literacy by asking basic questions to measure understanding of concepts. Almost one third of college graduates answer some of these questions incorrectly, signifying a high proportion of financial illiteracy across the board. According to Lusardi and Mitchell (2005), those who understand financial concepts including inflation, compound interest, risk diversification, or stock risk, make better choices, such as effective investment choices. Additionally, those with higher financial literacy have greater wealth accumulation, even when controlling for other determinants of wealth, such as income, age, education, family composition, risk tolerance patience, and saving behavior. Van Rooij, et al. (2011) believe this occurs because heightened financial knowledge reduces the barriers to gathering and processing information and increases involvement in the stock market. This connection between financial literacy and financial behavior highlights the importance of promoting knowledge and motivation in order to encourage better health- or money-related decisions.
Health literacy directly affects health outcomes, some of which bear financial consequences, both on patients and on the health care and welfare systems. Even when adjusting the analyses for socioeconomic status, health status, and health behaviors, Medicare enrollees with low health literacy had higher hospitalization rates (Baker et al. 2007). The American Medical Association (AMA) estimates that individuals with limited health literacy incur medical expenses that are up to four times greater than patients with adequate literacy skills, costing the health care system billions of dollars every year in unnecessary doctor visits and hospital stays (White 2008). Vernon, Trujillo, Rosenbaum, and DeBuono (2007) estimate that limited health literacy will cost the nation between $100 and $200 billion a year.
Improving health literacy would result in higher levels of efficiency, reduced collection costs, and consequently, improved bottom lines for medical institutions. As an analogy, financial literacy programs are fast becoming a key ingredient in financial policy reform worldwide (Xu and Bilal 2012). Similarly, the promotion of health literacy is in the best interest of both individuals and institutions.
The remainder of this chapter has the following organization. The next section provides a brief discussion of the need for better control of chronic diseases. Next the chapter explains the relevance using a scorecard approach followed by a discussion of its advantages. Attention then focuses on the Take Care scorecard before introducing considerations for developing health and financial literacy scorecards and discussing their limitations. The penultimate section sets forth implications for financial literacy. The final section provides a summary and conclusions.
THE NEED FOR BETTER CONTROL OF CHRONIC DISEASES
This chapter proposes a digital health scorecard to help prevent chronic disease (e.g., diabetes, cardiovascular diseases, and cancer). These are among the most prevalent, costly, and preventable of all health problems (Clark 2003). The Sixty-sixth United Nations General Assembly (September 19, 2011) proclaimed the spread of non-communicable diseases (i.e., chronic, noncontagious) as a socioeconomic and development challenge of epidemic proportions. Preventing diseases before they start is one of the most commonsense ways to keep people healthy at relatively low costs. The Robert Wood Johnson Foundation president and chief executive officer (CEO) maintains that instead of focusing on treating disease, people should be kept out of the doctor's office in the first place by investing in proven, community-based prevention efforts (Lavizzo-Mourey 2012). Most pertinent to this chapter is the fact that chronic diseases are increasingly self-managed by the patient, resulting in reduced hospitalizations, emergency department use, and overall managed care costs (Coleman, Thoesen, and Newton 2005).
A growing body of evidence supports the advantages of self-management and patient participation approaches in terms of knowledge, performance of self-management behaviors, monitoring, self-efficacy, health care use, and aspects of health status (Lorig et al. 1999). Patient participation has been recognized as a crucial element in chronic disease prevention (Institute of Medicine 2001), and interventions incorporating self-management had the most positive outcomes (Barlow et al. 2010). Still, patients are often reluctant to take part in decision-making processes, perhaps because they feel ill-equipped to deal with medical information. Yet, this can be countered by presenting information in a clear and understandable way, and interventions such as using decision aids to inform patients of decision options lead to a dramatic increase in participation (Van Tol-Geerdink et al. 2006).
Similar to patient participation, which occurs more often when patients feel knowledgeable about their health and the impact of the choices they make, connections exist between financial literacy and financial planning. Lusardi and Mitchell (2005) find that financially literate populations (assessed through ability to answer three questions on compound interest, inflation, and stock risk) have much higher rates of retirement planning. Retirement planning also requires using tools such as financial calculators. The authors also note that people with higher financial literacy are more likely to use these tools and plan efficiently. Further, financial instruction should include not only focus on subject matter-related material, but also links to implementation (Hill, Meszaros, and Yetter 2012). All this supports the need for a simple tool to make health knowledge widely accessible and actionable and a financial literacy tool to follow.
THE SCORECARD APPROACH
To better address the need for a brief, easily comprehensible and widely accessible self-management tool for prevention and monitoring of chronic disease, a general-purpose digital health scorecard is proposed. This user-friendly, efficient tool focuses on key indicators to help consumers understand how to optimize health behaviors in terms of medical testing and lifestyle. Alongside promoting disease prevention and management, the scorecard is an education tool. Users learn what healthy behaviors are and what their numbers for indicators such as blood pressure should be based on the values presented on the scorecard. Additionally, users discover their problem areas and the choices they can make to positively affect their health.
Yates and Ward (2012) propose a similar approach for financial literacy, rating it, interestingly, from being in “excellent health” to “moderately healthy” to “unhealthy.” The authors find that while most people are knowledgeable about credit cards and mortgages, knowledge varies substantially across topics. For example, people often mishandle estate planning and emergency funds. Individuals appear to be aware of what they do not know, and many point to the latter topics as ones about which they would like to become more knowledgeable.
Mandell and Schmid Klein (2009) study individuals from one school district, who either did or did not choose to take a course in personal financial management when they were in high school. Of the 79 respondents, about half took the course, with college-bound students no more likely to take it than other students. In their follow-up study, the authors find that those who took the course did not consider themselves to be more savings-oriented than those who did not take the course, nor did they report better financial behavior than those who did not take the course. While Mandell and Schmid Klein find positive financial behavior associated with respondents who were full-time college students or graduates, their results are driven by paying credit cards in full and the belief that their savings and investments are adequate for their needs. This might suggest that minimal training, in several basic aspects of prudent financial behavior, would suffice, as more elaborate training did not have meaningful outcomes. Such minimal training is in line with the scorecard approach and could be more beneficial when administered to adults, who are already managing their own finances, than to high school students.
Studies show that a majority of patients prefer to receive numerical information as part of their care (Wallsten et al. 1993). Such major organizations as the Mayo Clinic staff have developed paper-based health scorecards designed to address this need. Even more promising are scorecards that use Interactive Health Communication Applications (IHCAs) for the user to access or transmit health information or receive guidance and support on a health-related issue (Adler et al. 1998). IHCAs have a significant positive effect on knowledge, perceived social support, health behaviors, and clinical outcomes, and may have a positive effect on self-efficacy (Murray, Burns, See Tai, Lai, and Nazareth 2005). Still, most (73 percent) technology-based interventions require therapist involvement (Rosser et al. 2009). Because the proposed digital scorecard would not require a comprehensive medical assessment, the consumer can see which behaviors and biochemical markers contribute to a better score and are thus linked to improved health status.
TARGET POPULATION AND ADVANTAGES
Besides promoting action in patients with chronic disease, the scorecard can be used to promote disease prevention among healthy people who want to assess or maintain their health status. A report by the Pew Internet and American Life Project reveals that in 2009, 61 percent of American adults looked online for health information, with more than 90 percent of them seeking material related to illnesses (Fox and Jones 2009). However, a need still exists for online material to motivate action or nudge individuals toward healing and prevention.
Preliminary surveys taken by Carnegie Mellon University students, faculty, and staff show that even educated populations are unaware of what is considered healthy behavior and numbers, and should also be targeted by this intervention (Bhavnani et al. 2011). A later section addresses the full results of this study. By harnessing technology, a digital scorecard has the potential to control chronic illness and provide health information to people all over the world. Even a single use of the tool is important in teaching the consumer how to live a healthier lifestyle, which may lead to changes, even if they are relatively minor. The surveys from Carnegie Mellon reveal that the simplicity of the scorecard would appeal to a variety of populations.
Because the scorecard has a greater ability to be a learning tool than other similar tools currently on the market, it is more likely to inspire change (Bhavnani et al. 2011). The most prominent feature of the proposed digital Take Care scorecard is its ability to capture an individual's overall health (or preventable disease risk) with a single, easily comprehensible number and a guideline for interpretation with clear implications. Thus, the scorecard focuses on the major determinants of health and is easily comprehensible rather than encumbered by medical jargon.
CONTENT OF THE TAKE CARE SCORECARD
A digital scorecard can display a person's ratings on several basic health measures associated with preventable disease. As Exhibit 17.1 shows, the Take Care scorecard includes body mass index (BMI), blood sugar, blood pressure, and cholesterol levels, as well as behavioral factors such as smoking and exercise. The scorecard provides recommended actions on each health measure, allowing users to keep track of their health and monitor risk factors. The inclusion of the recommending sources suggests a convergence of recommendations.
Exhibit 17.1 Recommendations for Preventing Chronic Disease

Converging evidence for the seven health indicators included in the Take Care scorecard comes from research suggesting that glucose control (individualized for type 2 diabetic patients), smoking cessation, aspirin use, blood pressure, and LDL control are an effective multi-factorial therapy for reducing diabetes complications (Cleary et al. 2006). As Miron-Shatz and Ratzan (2011) point out, as few as five lifestyle factors—smoking, alcohol use, diet, body mass index, and physical activity—account for a 58 percent reduction in risk of developing pancreatic cancer and are related to diabetes incidence in 90 percent of new cases. These same factors are also related to recommended interventions for other diseases such as cardiovascular illness (Mayo Clinic Staff 2011). Because the health indicators included in the proposed scorecard are key variables for many chronic diseases, the scorecard use may result in better control of a variety of chronic conditions. A key determinant for including an indicator in the scorecard is simple measurability and comprehensibility. Although a healthy diet is a key variable (Mayo Clinic Staff 2011), it was not included because a healthy diet is complex to explain, varies across people, and is difficult to measure (Canoy and Buchan 2007).
CONSIDERATIONS FOR HEALTH AND FINANCIAL LITERACY SCORECARDS
An overall health score is computed that is well-suited for evaluation, surveillance, and comparison across multiple locations and populations. As Exhibit 17.2 shows, the score is computed as the total number of health indicators within the healthy (goal) range provided alongside each indicator. The proposed digital scorecard includes a continuous composite overall health score along with score ranges and a brief action-oriented interpretation of this score (0–4, “Take care!”; 5–6, “Getting there”; and 7, “Excellent”). Using a composite score that integrates multiple measurements has key advantages, including increased validity by providing a more representative sample of information about the underlying concept and increased precision by decreasing score variability (Stewart, Hays, and Ware 1992). These same considerations can serve when creating a scorecard for financial literacy.
Exhibit 17.2 The Proposed Health Scorecard: “Take Care—7 Steps for Better Health”
Note The Take Care scorecard allows users to evaluate their health in a simple way and to learn the targets they should be aiming for to improve health.

The scorecard embodies knowledge translation, an emerging concept in medical practice and interventional epidemiology (Davis et al. 2003). Translational medicine aims to optimize patient care by entering the realm of lifestyle practices. The proposed scorecard is designed to improve health by promoting healthy behaviors in consumers' daily routines. Further, consumers may share their scorecard information with physicians, enabling them to better monitor progress and develop an optimal treatment plan.
To help overcome barriers to health literacy and create motivation for health improvement, the Take Care scorecard is designed according to recommendations for health literacy enhancement interventions, including provision of simplified (Miron-Shatz et al. 2011) and more attractive written materials (Apfel et al. 2010). Recommended formats are those with more white space, friendlier layout, short sentences, simple words, and large fonts (Apfel et al. 2010). Also recommended is text that is action- and goal-oriented, with a clear explanation of its purpose.
Both the scorecard and the lowest of the score ranges are named Take Care as an affective cue to spur the consumer to action. Taking care of oneself implies cautious and responsible action, and the phrase is commonly used to wish others well. Researchers document the importance of affect in information processing and decision-making (Zajonc 1980; Bechara et al. 1997; Loewenstein et al. 2001). People often base their judgment on emotional cues, if present (Slovic et al. 2002). These findings suggest that emotionally charged language may increase usage and perceived benefit. Finally, theoretical frameworks underlying behavior change interventions in chronic illness (e.g., cognitive behavioral therapy) generally suggest that internal events, such as self-efficacy and motivation, should be the primary target of intervention (Rosser et al. 2009). Bearden and Haws (2012) find that low self-control often underlies many consumer decisions. This result emphasizes the role of motivation in promoting decision-making that would serve the individual's long-term goals. For example, self-control bias leads consumers to think that their self-control is greater than it really is, and to trust themselves to eventually save enough for retirement. Yet, this bias will lead consumers to spend more money today, at the cost of saving for retirement in the future, while at the same time being fairly confident that this saving will occur.
All these principles pertaining to presentation of information, motivating users, and creating a sense of self-efficacy are also highly pertinent to financial decision-making. Further, lessons from a financial literacy program for students (Carlin and Robinson 2010) highlight the importance of including several criteria for knowledge: Students who received training tend to save more today, but their ability to make trade-offs between current costs and future benefits is somewhat impaired. As Kaenzig and Wüstenhagen (2010) show, consumer investment decisions for products and services with higher initial costs and lower operating costs are potentially subject to numerous cognitive biases, such as present-biased preferences or framing effects. Lynch et al. (2010) expand this to claim that consumers' financial illiteracy is apparent in major financial decisions involving time trade-offs, such as mortgages, retirement savings, and decumulation of savings in retirement.
Sharpe (2008, p. 328) points out that these tradeoffs also exist in health insurance, as: “Compared with those who have comprehensive health insurance, consumers with high deductible plans are more likely to economize on health care services. But, they are also more likely to delay or avoid necessary care.” This suggests that a comprehensive scorecard approach can also be beneficial for investment and financial decisions in the health domain and in general.
The principles implemented in the scorecard also allow it to “nudge” the user toward making better decisions related to healthy lifestyles. Nudging, as defined by Thaler and Sunstein (2009, p. 6), is “alteration of people's behavior in a predictable way without forbidding any options or significantly changing economic incentives.” Researchers also examine this approach and its ethical principles regarding health decisions (Blumenthal-Barby, Swindell, and Burroughs 2012). The scorecard's actionable language and presentation of information is meant to alter behavior so that users make more informed decisions about their health care and lifestyle choices to prevent chronic diseases. According to Thaler and Sunstein, many smokers, drinkers, and overeaters are willing to pay for decision aids to nudge them into making better decisions for their health. With a digital scorecard, this could be provided in a free and easy-to-use fashion.
A study on the effect of monetary incentives on weight loss programs tests theories of behavioral economics that indicate the potential effectiveness of a scorecard approach. Volpp et al. (2008) provide financial incentives for participants who achieve their weight loss goals, either consistently every time they weigh in on target or in a lottery system approach. Their study shows that incentive groups lose more weight on average than the control groups, and some key behavioral economic concepts emerge that pertain to the scorecard approach. Rapid feedback, as would be provided by the scorecard, fosters greater adherence to the weight loss program. The patient-centered scorecard gives users immediate feedback on their health status and ways to achieve better health.
Prior studies show that offering incentives to the participant rather than a physician is more likely to create behavior change. If users understand the many financial benefits of healthy lifestyles and improved health literacy, they will see the substantial financial incentives involved with adherence to the scorecard. However, Adams (2010) calls for more research on the long-term effects of behavioral economics and whether behavior change can be influenced in the long term. The appropriate use of the scorecard, on multiple occasions and in collaboration with a physician, can provide a nudge that can have lasting effects on health outcomes.
Although the main purpose of the Take Care scorecard is to improve health, it is also associated with other enduring benefits, perhaps most importantly to create a clear mental model of health. This involves a patient's set of concepts, ideas, beliefs, and values about what health is and what it means (Galt 2006), which even patients diagnosed with a chronic disease do not necessarily have. For example, about 60 percent of hypertensive patients do not know that exercise lowers blood pressure (Williams et al. 1998). Similarly, two out of three people with diabetes do not consider cardiovascular disease a significant risk factor (U.S. Department of Health and Human Services 2002).
Researchers recommend that preventive programs and public awareness messages educate patients about health indicators and their associated risks to minimize diabetes complications and healthcare costs (Okoro et al. 2004). The analogy to financial decision-making is clear—creating a mental model of good financial health is not a trivial task. Helping consumers understand that annual percentage rates (APR) and credit scores, as well as savings and retirement plans, are part of proper financial management, are important and worthy goals that a financial scorecard could accomplish.
Holtgrave and Weber (1993) compare two models of risk perception for both financial and health risk stimuli (such as radon gas exposure, and investing 80 percent of one's fortune in medical research). They find that a model inspired by Luce and Weber's Conjoint Expected Risk (CER) using dimensions of probability of gain, loss and status quo, and expected benefit and harm provide the best fit for most subjects and stimuli. The researchers presume that similar approaches underlie risky activities in health and finances. Incorporating a factor of dread related to health risks improved the explanatory power of their model. This attests to the proximity of health and financial judgments and to the potential benefit from cross-learning.
Preliminary Testing and Support for the Scorecard Idea
A pilot project at Carnegie Mellon University shows the true potential of a scorecard approach to health literacy and chronic disease prevention. Graduate students at Carnegie Mellon's Heinz College, School of Public Policy and Information Systems, conducted surveys of health literacy among college-educated students and designed and developed a prototype for an online scorecard (Bhavnani et al. 2011).
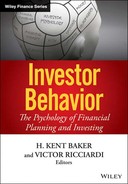
Surveys of over 200 Heinz College students, staff, and faculty assessed knowledge of BMI, blood pressure, blood sugar, cholesterol, smoking, exercise, and alcohol, both knowledge of the normal healthy range and awareness of a person's own value. In spite of high health literacy, only 11.9 percent of participants knew their blood sugar levels, and 22.7 percent knew the healthy range. Few participants (15.9 percent) knew their cholesterol levels, while 38.3 percent knew the normal range. All participants (100 percent) knew their values for the behavioral indicators—smoking, exercise, and alcohol intake—but only 36.6 percent knew the appropriate amount of exercise necessary for a healthy lifestyle, and 65.5 percent knew the healthy amount of alcohol intake. Most importantly, a majority (73.6 percent) of survey participants expressed interest in using a digital scorecard for regularly tracking their health status (Bhavnani et al. 2011). Exhibit 17.3 displays these results.
Exhibit 17.3 Carnegie Mellon Survey Results of Personal Knowledge of Chronic Disease Indicators
| Health Indicators | % Who Knew Their Own Value | % Who Knew the Normal Range |
| BMI | 49.30 | 58.70 |
| Blood pressure | 59.70 | 54.70 |
| Blood sugar | 11.90 | 22.70 |
| Cholesterol | 15.90 | 38.30 |
| Smoking | 100.00 | 98.50 |
| Exercise | 100.00 | 36.60 |
| Alcohol | 100.00 | 65.50 |
| Note This exhibit shows that in a survey of student and faculty at Carnegie Mellon, people are unaware of their numbers involving their health. | ||
These numbers demonstrate a low level of health knowledge, even in educated populations. This highlights the potential for the scorecard to provide actionable knowledge, thereby hopefully reducing the prevalence of chronic diseases. The prototype website, called “Score Your Health,” allowed users to input their information and calculate a comprehensive score showing which of the seven areas the user needed to improve. The low literacy levels coupled with high interest in a scorecard demonstrate the scorecard can prove to be a powerful tool in chronic disease prevention.
The survey also reveals some qualities of a health assessment tool that survey participants felt would most promote widespread use, and the scorecard would be able to achieve all these qualities. Most respondents (77.2 percent) report that simplicity would be the feature most likely to make them use the application, and 59.1 percent note ease in understanding the tool (Bhavnani et al. 2011). Again, this suggests that any scorecard should use a format that promotes simplicity and comprehension, such as the short, action-oriented sentences and friendly formats proposed by Apfel et al. (2010).
To assess strengths and weaknesses of the simplified digital scorecard approach, Carnegie Mellon graduate students compared it with several similar health assessment tools (Bhavnani et al. 2011). The strengths of the scorecard, which all received the maximal ratings, include the ability to teach how to make healthy decisions, speed of use, detailed and actionable feedback, promoting learning after use, objectivity, and being easily understandable. Some weaknesses are credibility and ability to teach about a specific health risk (Bhavnani et al. 2011). With time and use, credibility of the scorecard can increase. Compared to the average values calculated for the five other health tools assessed at Carnegie Mellon, the scorecard approach appears to exceed existing tools in teaching the user how to make healthy decisions, tracking healthiness, promoting self-improvement, speed of use, giving actionable feedback, promoting learning while taking the quiz and after, and ease of understanding (Bhavnani et al. 2011). Exhibit 17.4 displays the comparison of the Take Care scorecard with the other instruments.
Exhibit 17.4 Graphical Representation of Market Strengths and Weaknesses of the Scorecard
Note: This exhibit shows that compared to other scorecards, the Take Care scorecard is better at tracking individual healthiness, promoting learning, teaching healthy decision-making, providing detailed and actionable feedback, and portraying objectivity.

LIMITATIONS
Scorecards may oversimplify health information and may be inappropriate for a minority of consumers (van Tol-Geerdink et al. 2006). However, Ratzan (2009) suggests that the benefits of greater ease of use and interpretability far outweigh the risk of oversimplification. Further, for consumers who want to fully understand the evidence underlying their score, supplementary material would be provided online, including graphical representations of the scores and access to evidence-based studies supporting the indicators presented similar to the format of the Cochrane Collaboration (Higgins and Green 2011).
IMPLICATIONS FOR FINANCIAL LITERACY
Health literacy and financial literacy are linked, as recently documented by a study of adults without dementia. Results agree with prior studies showing that poor health literacy results in lower overall health, but financial literacy also correlates with health status and behavior. Research shows positive correlations between numeric abilities and financial literacy, and health outcomes, defining better health status in terms of cognitive function, physical activity, and mental health (Bennett et al. 2012). This leads to the conclusion that higher rates of both health and financial literacy are necessary for improved health status.
In creating an Economic Stability Index (ESI), Hacker et al. (2012) include medical spending as a large consideration. According to Hacker et al. (2012, p. 5), the ESI measures the “degree to which individuals are protected against hardship-causing economic losses.” The authors also note that medical-out-of-pocket spending is often a large risk for economic losses and one of the biggest worries of economic risk for Americans. Miron-Shatz (2009) also shows that finances are intertwined with health and well-being: Women who consider their finances when thinking about the future are less happy than those who do not spontaneously think about it. This may underlie the correlation between financial literacy and mental health status seen by Bennett et al. (2012). As Hacker et al. (2012, p. 12) note, the ESI is meant to help in defining precautionary savings as a “financial safety net.” To calculate this safety net for health care, consumers would require improving their literacy—health and financial.
Sharpe (2008) calls for economists to help facilitate a better understanding of the health care market. Consumers cannot process health information and therefore sometimes go without health care. Sharpe (2008, p. 330) poses a question that is central to health literacy: “What changes in information delivery might help the consumer better understand and use highly technical and complex health information?” This chapter contends that a great need exists for improved health literacy and suggests using a scorecard approach as a tool to reduce chronic diseases and the economic burden of medical expenses. A similar need exists for financial literacy and a scorecard approach could help to fill this gap.
Currently, no standardized tool is widely used to measure financial literacy (Huston 2010). However, experts have created some simple tools such as Lusardi and Mitchell's (2005) use of three questions to assess financial literacy levels. In fact, a lack of agreement exists among studies for even a standard definition of financial literacy. As Huston notes, only eight (13 percent) studies of financial literacy in the past 10 years defined the term at all. Two of these used only financial knowledge as a definition, three referred to abilities, and two used both knowledge and ability in the definitions. Content areas of the studies of financial literacy could be divided into four categories: knowledge of money basics, borrowing, investing, and protecting resources. Most studies do not contain an indicator for whether the study participant is financially literate. A formalized definition and tool to assess financial literacy, as well as for education programs to improve the status of financial literacy in the public, are overdue. According to Way and Wong (2010) choice architecture, or nudging, can serve as a potentially successful tool for increasing both financial and health literacy. A scorecard approach to financial literacy can achieve all these goals.
Adopting a digital, standardized assessment tool for financial literacy can also serve educational purposes. For example, a website similar to the “Score Your Health” prototype can be created, asking simple financial literacy questions, rating the user's financial literacy level, explaining the questions answered incorrectly, and linking to resources that may help the user learn more about the topics questioned. Bases for creating the scorecard include trends found in recent financial literacy studies, the four content areas of financial literacy, and a standardized definition of financial literacy. The key to improving literacy levels is creating user-friendly tools that will encourage the participants to want to increase their scores. As Bertrand, Mullainathan, and Shafir (2006) suggest, future developments of the financial literacy scorecard should take into account specific populations' needs and decision-making considerations, including those at all income/wealth levels. In fact, other work (Bryan et al. 2012) shows that the beneficial association between literacy (both health and financial) and health care decision-making is stronger among those who are older, poorer, and at the lower ranges of cognitive ability. Because higher levels of health and financial literacy are associated with better decision-making (Hanoch et al. 2010), improvements in literacy could facilitate better decision-making and lead to improved quality of life in later years.
SUMMARY
This chapter proposes a succinct and actionable approach to overcoming health literacy barriers, thereby improving decision-making and ultimately preventing or curbing chronic disease and easing the medical and economic burden. A similar approach is proposed for improving financial decision-making, and, ultimately, outcomes. In the health domain, although patient participation is a key element in chronic disease prevention and improved outcomes, patients are often reluctant to participate.
The chapter presents a digital self-management tool for prevention and monitoring of chronic disease called the Take Care health scorecard. The scorecard captures overall health or preventable disease risk with a single number and a guideline with clear implications. It also promotes literacy by creating a clear mental model of health. In a pilot study, the majority of participants expressed interest in using a digital scorecard for regular monitoring of health status and most often rated simplicity and ease of use as the most important features of such a tool (Bhavnani et al. 2011).
In the financial domain, financial literacy is important to effective financial planning, including better investment choices and greater wealth accumulation. Yet, college graduates and others often do not understand basic financial concepts. Way and Wong (2010) show that user-friendly tools encouraging participants to increase their scores lead to improved literacy. Moreover, both health and financial literacy share risk perception dimensions involving the probability of gain, loss, and status quo and expected benefit and harm (Holtgrave and Weber 1993). Additionally, financial literacy is correlated not only with health status and behavior but also with happiness. Thus, developing a scorecard to improve financial literacy may also lead to comprehensive well-being. This is a good example of how interventions at the micro level can have a lasting effect on economic outcomes.
DISCUSSION QUESTIONS
1. Despite being intuitively appealing, what are some objections to a health scorecard approach?
2. Who should apply a scorecard approach?
3. Discuss whether a scorecard approach can be appropriate for financial literacy or whether it is too simplistic.
4. What concepts should be included in a financial literacy scorecard?
5. How could a financial literacy scorecard best be used to better a population's understanding of financial concepts?
REFERENCES
Adams, Robert John. 2010. “Improving Health Outcomes with Better Patient Understanding and Education.” Risk Management and Healthcare Policy 3:61, 61−72.
Adler, Linda, Farrokh Alemi, David G. Ansley, Patricia F. Brennan, Molly Joel Coye, David Gustafson, Joseph Henderson, Holly Jimison, Albert Mulley, John Noell, Kevin Patrick, Thomas C. Reeves, Thomas Robinson, and Victor Strecher. 1998. Science Panel on Interactive Communication and Health Summary Statement. Washington, DC: Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services. Available at http://odphp.osophs.dhhs.gov/confrnce/partnr98/SciPICH.htm.
American College of Cardiology Foundation. 2011a. “Am I at Risk?” Available at www.cardiosmart.org/CardioSmart/AmIAtRisk.aspx.
American College of Cardiology Foundation. 2011b. “Learn about Heart Disease.” Available at www.cardiosmart.org/heartdisease/cttbrowser.aspx?category=risk%20factors.
American Heart Association. 2011. “Life's Simple 7: Heart Health Factors.” Available at http://mylifecheck.heart.org/Multitab.aspx?NavID=3.
Apfel, Franklin, Kara L. Jacobson, Ruth M. Parker, Julia Taylor, Tony Boyle, Joanna Groves, Jeremiah Mwangi, Scott Ratzan, and Carinne Allison. 2010. Health Literacy: Action and Guide Part 2: Evidence and Case Studies. Axbridge, UK: World Health Communication Associates Ltd. Available at www.whcaonline.org/uploads/publications/WHCAhealthLiteracy-28.3.2010.pdf.
Baker, David W., Michael S. Wolf, Joseph Fienglass, Jason A. Thompson, Julie A. Gazmararian, and Jenny Huang. 2007. “Health Literacy and Mortality among Elderly Persons.” Archive of Internal Medicine 167:14, 1503−1509.
Barlow, Cate, Debbie Cooke, Kathleen Mulligan, Eric Beck, and Stanton Newman. 2010. “A Critical Review of Self-Management and Educational Interventions in Inflammatory Bowel Disease.” Gastroenterology Nursing 33:1, 11−18.
Bearden, William O., and Kelly L. Haws. 2012. “How Low Spending Control Harms Consumers.” Journal of the Academy of Marketing Science 40:1, 181−193.
Bechara, Antoine, Hanna Damasio, Daniel Tranel, and Antonio R. Damasio. 1997. “Deciding Advantageously before Knowing the Advantageous Strategy.” Science 275:5304, 1293–1295.
Bennett, Jarred S., Patricia A. Boyle, Bryan D. James, and David A. Bennett. 2012. “Correlates of Health and Financial Literacy in Older Adults without Dementia.” BMC Geriatrics 12 (June 12): 30−39. Available at www.biomedcentral.com/1471-2318/12/30.
Bertrand, Marianne, Sendhil Mullainathan, and Eldar Shafir. 2006. “Behavioral Economics and Marketing in Aiding Decision Making Among the Poor.” Journal of Public Policy & Marketing 25:1, 8–23.
Bhavnani, Ashwin, Rebecca Tyrrell, Emily Allen, Won Dechpinya, Yun Gao, and Yasaman Torabi. 2011. “Design, Implementation, and Go-To Market Strategy for the Digital Health Scorecard: A Social Marketing Approach to Health Literacy.” Unpublished manuscript, Carnegie Mellon University.
Blumenthal-Barby, Jennifer Swindell, and Hadley Burroughs. 2012. “Seeking Better Health Care Outcomes: The Ethics of Using the ‘Nudge'.” American Journal of Bioethics 12:2, 1−10.
Bryan, D. James, Patricia T. Boyle, Jarred S. Bennett, and David A. Bennett. 2012. “The Impact of Health and Financial Literacy on Decision Making in Community-Based Older Adults.” Gerontology 58:6, 531−539.
Carlin, Bruce Ian, and David T. Robinson. 2010. What Does Financial Literacy Training Teach Us? National Bureau of Economic Research, No. w16721. Available at www.nber.org/papers/w16271.pdf?new_window=1.
Canoy, Dexter, and Iain Buchan. 2007. “Challenges in Obesity Epidemiology.” Obesity Reviews 8:Supplement 1, 1–11.
Cleary, Patricia A., Trevor J. Orchard, Saul Genuth, Nathan D. Wong, Robert Detrano, Jye-Yu C. Backlund, Bernard Zinman, Alan Jacobson, Wanjie Sun, John M. Lachin, and David M. Nathan. 2006. “The Effect of Intensive Glycemic Treatment on Coronary Artery Calcification in Type 1 Diabetic Participants of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study.” Diabetes 55:12, 3556–3565.
Clark, Noreen M. 2003. “Management of Chronic Disease by Patients.” Annual Review of Public Health 24 (1): 289–313.
Coleman, Mary Thoesen, and Karen S. Newton. 2005. “Supporting Self-Management in Patients with Chronic Illness.” American Family Physician 72:8, 1503–1510.
Davis, Dave, Mike Evans Davis, Alex Jadad, Laure Perrier, Darlyne Rath, David Ryan, Gary Sibbald, Sharon Straus, Susan Rappolt, Maria Wowk, and Merrick Zwarenstein. 2003. “The Case for Knowledge Translation: Shortening the Journey from Evidence to Effect.” BMJ 327:7405, 33–35.
Fox, Susannah, and Sydney Jones. 2009. The Social Life of Health Information. Washington, DC: Pew Internet and American Life Project. Available at www.pewinternet.org/~/media//Files/Reports/2009/PIP_Health_2009.pdf.
Galt, Kimberly A. 2006. Developing Clinical Practice Skills for Pharmacists. Bethesda, MD: American Society of Health-System Pharmacists.
Hacker, Jacob S., Gregory Huber, Austin Nichols, Philip Rehm, Mark Schlesinger, Craig Stuart, and Robert G. Valletta. 2012. “The Economic Security Index: A New Measure for Research and Policy Analysis.” Working Paper 2012-21, Federal Reserve Bank of San Francisco. Available at www.frbsf.org/publications/economics/papers/2012/wp12-21bk.pdf.
Hanoch, Yaniv, Talya Miron-Shatz, Helen Cole, Mary Himmelstein, and Alex D. Federman. 2010. “Choice, Numeracy and Physicians-in-Training Performance: The Case of Medicare Part D.” Health Psychology 29:4, 454−459.
Harvard Medical School. 2010. “American Ideal.” Harvard Heart Letter, April. Available at https://www.health.harvard.edu/newsletters/Harvard_Heart_Letter/2010/April/american-ideal.
Higgins, Julian P. T., and Sally Green, eds. 2011. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Available at www.cochrane-handbook.org.
Hill, Andrew T., Bonnie T. Meszaros, and Erin A. Yetter. 2012. “The Keys to Financial Success Curriculum: Impact on Personal Finance Behaviors.” Working Paper, Federal Reserve Bank, Philadelphia. Available at www.aeaweb.org/aea/2012conference/program/retrieve.php?pdfid=608.
Holtgrave, David R., and Elke U. Weber. 1993. “Dimensions of Risk Perception for Financial and Health Risks.” Risk Analysis 13:5, 553–558.
Huston, Sandra J. 2010. “Measuring Financial Literacy.” Journal of Consumer Affairs 44:2, 296–316.
Institute of Medicine. 2001. “Improving the 21st-Century Health Care System.” In Rona Briere, ed., Crossing the Quality Chasm, 61–88. Washington, DC: The National Academies Press.
Kaenzig, Joseph, and Rolf Wüstenhagen. 2010. “The Effect of Life Cycle Cost Information on Consumer Investment Decisions Regarding Eco-Innovation.” Journal of Industrial Ecology 14:1, 121–136.
Lavizzo-Mourey, Risa. 2012. “We Must Focus on Preventing Disease If We Want Our Nation to Thrive.” The Atlantic. Available at www.theatlantic.com/health/archive/2012/05/we-must-focus-on-preventing-disease-if-we-want-our-nation-to-thrive/257759/.
Loewenstein, George F., Elke U. Weber, Christopher K. Hsee, and Ned Welch. 2001. “Risk as Feelings.” Psychological Bulletin 127:2, 267–286.
Lorig, Kate R., David S. Sobel, Anita L. Stewart, Byron William Brown, Jr., Albert Bandura, Philip Ritter, Virginia Gonzalez, Diana D. Laurent, and Halstead R. Holman. 1999. “Evidence Suggesting that a Chronic Disease Self-Management Program Can Improve Health Status While Reducing Hospitalization: A Randomized Trial.” Medical Care 37:1, 5–14.
Lusardi, Annamaria, and Olivia S. Mitchell. 2005. “Financial Literacy and Planning: Implications for Retirement Wellbeing.” University of Michigan Retirement Research Center.
Lynch, John G. Jr., Richard G. Netemeyer, Stephen A. Spiller, Stephen A., and Alessandra Zammit. 2010. “A Generalizable Scale of Propensity to Plan: The Long and the Short of Planning for Time and for Money.” Journal of Consumer Research 37:1, 108−128.
Mandell, Lewis, and Linda Schmid Klein. 2009. “The Impact of Financial Literacy Education on Subsequent Financial Behavior.” Journal of Financial Counseling and Planning 20:1, 15−24.
Mayo Clinic Staff. 2011. “5 Medication-Free Strategies to Help Prevent Heart Disease.” Mayo Foundation for Medical Education and Research (MFMER), January 12. Available at www.mayoclinic.com/health/heart-disease-prevention/WO00041/METHOD=print.
Miron–Shatz, Talya. 2009. “Am I Going to Be Happy and Financially Stable?”: How American Women Feel When They Think about Financial Security.” Judgment and Decision Making 4:1, 102–122.
Miron–Shatz, Talya, Yaniv Hanoch, Dana Graef, and Michal Sagi. 2009. “Presentation Format, Numeracy, and Emotional Reactions: The Case of Prenatal Screening Tests.” Journal of Health Communication 14:5, 439–450.
Miron-Shatz, Talya, Ingrid Mühlhauser, Bruce Bower, Michael Diefenbach, Ben Goldacre, Richard S. W. Smith, David Spiegelhalter, and Odette Wegwarth. 2011. “Barriers to Health Information and Building Solutions.” In Gerd Gigerenzer and J. A. Muir Gray, eds., Better Doctors, Better Patients, Better Decisions: Envisioning Healthcare 2020, Strüngmann Forum Report Volume 6, 191–214. Cambridge: MIT Press.
Miron-Shatz, Talya, and Scott Ratzan. 2011. “The Potential of an Online and Mobile Health Scorecard for Preventing Chronic Disease.” Journal of Health Communication 16:2, 175−190.
Mozaffarian, Dariush, Aruna Kamineni, Mercedes Carnethon, Luc Djoussé, Kenneth J. Mukamal, and David Siscovick. 2009. “Lifestyle Risk Factors and New-Onset Diabetes Mellitus in Older Adults: The Cardiovascular Health Study.” Archive of Internal Medicine 169:8, 798−807.
Murray, Elizabeth, Joanne Burns, Sharon See Tai, Rosalind Lai, and Irwin Nazareth. 2005. “Interactive Health Communication Applications for People with Chronic Disease.” Cochrane Database of Systematic Reviews 4, CD004274.
National Institutes of Health. 2011. Brain Basics: Preventing Stroke. Bethesda, MD: Office of Communication and Public Liaison, National Institute of Neurological Disorders and Stroke. NIH Publication No. 11-3440b. Available at www.ninds.nih.gov/disorders/stroke/Brain_Basics-Preventing_Stroke_brochure.pdf.
Okoro, Catherine A., Ali H. Mokdad, Earl S. Ford, Barbara A. Bowman, Frank Vinicor, and Wayne H. Giles. 2004. “Are Persons with Diabetes Practicing Healthier Behaviors in the Year 2001? Results from the Behavioral Risk Factor Surveillance System.” Preventive Medicine 38:2, 203–208.
Ratzan, Scott C. 2009. “Integrating Health Literacy into Primary and Secondary Prevention Strategies.” Institute of Medicine Workshop on Integrating Health Literacy into Primary and Secondary Prevention Strategies, September 15. Washington, DC: Institute of Medicine. Available at www.iom.edu/~/media/Files/Activity%20Files/PublicHealth/HealthLiteracy/2009-SEP-15/02-Ratzan.pdf.
Ratzan, Scott C., and Ruth M. Parker. 2000. “Introduction.” In National Library of Medicine Current Bibliographies in Medicine: Health Literacy. NLM Pub. No. CBM 2000-1. Bethesda, MD: National Institutes of Health, U.S. Dept. of Health and Human Services.
Rosser, Benjamin A., Kevin E. Vowles, Edmund Keogh, Christopher Eccleston, and Gail A. Mountain. 2009. “Technologically-Assisted Behavior Change: A Systematic Review of Studies of Novel Technologies for the Management of Chronic Illness.” Journal of Telemedicine and Telecare 15:7, 327–338.
Sharpe, Deanna L. 2008. “Consumer Financial Issues in Health Care.” In Jing Jian Xiao, ed., Handbook of Consumer Financial Research, 318–355. New York: Springer.
Slovic, Paul, Melissa Finucane, Ellen Peters, and Donald G. MacGregor. 2002. “The Affect Heuristic.” In Thomas Gilovich, Dale Griffin, and Daniel Kahneman, eds., Heuristics and Biases: The Psychology of Intuitive Judgment, 397–420. Cambridge: Cambridge University Press.
Stewart, Anita L., Ron D. Hays, and John E. Ware, Jr. 1992. “Methods of Constructing Health Measures.” In Anita L. Stewart and John E. Ware, Jr., eds., Measuring Functioning and Well-Being: The Medical Outcomes Study Approach, 67–85. Durham, NC: Duke University Press.
Thaler, Richard H., and Cass R. Sunstein. 2009. Nudge: Improving Decisions about Health, Wealth, and Happiness. New Haven, CT: Yale University Press.
U.S. Department of Health and Human Services. 2002. “HHS, American Diabetes Association Renew Campaign to Help People with Diabetes Know Their Cardiovascular Risks: New ADA Survey Shows Many Know Little about Risks of Heart Disease, Stroke.” February 19. Available at http://archive.hhs.gov/news/press/2002pres/20020219.html.
Van Rooij, Maarten, Annamaria Lusardi, and Rob J. Alessie. 2011. “Financial Literacy, Retirement Planning, and Household Wealth.” The National Bureau of Economic Research. Available at www.nber.org/papers/w17339.
Van Tol-Geerdink, Julia J., Peep F. M. Stalmeier, Emile N. J. T. van Lin, Erik C. Schimmel, Henk Huizenga, Wim A. J. van Daal, and Jan-Willem Leer. 2006. “Do Prostate Cancer Patients Want to Choose Their Own Radiation Treatment.” International Journal of Radiation Oncology · Biology · Physics 66:4, 1105–1111.
Vernon, John A., Antonio Trujillo, Sara Rosenbaum, and Barbara DeBuono. 2007. “Low Health Literacy: Implications for National Health Care Policy.” Washington, DC: George Washington University School of Public Health and Health Services.
Volpp, Kevin G., Leslie K. John, Andrea B. Troxel, Laurie Norton, Jennifer Fassbender, and George Loewenstein. 2008. “Financial Incentive–Based Approaches for Weight Loss.” JAMA: The Journal of the American Medical Association 300:22, 2631−2637.
Wallsten, Thomas S., David V. Budescu, Rami Zwick, and Steven M. Kemp. 1993. “Preferences and Reasons for Communicating Probabilistic Information in Verbal or Numerical Terms.” Bulletin of the Psychonomic Society 31:2, 135–138.
Way, Wendy L., and Nancy Wong. 2010. “Harnessing the Power of Technology to Enhance Financial Literacy Education and Personal Financial Well-Being: A Review of the Literature, Proposed Model, and Action Agenda.” Working Paper 10-6, Center for Financial Security, University of Wisconsin, Madison.
White, Sheida. 2008. “Assessing the Nation's Health Literacy: Key Concepts and Findings of the National Assessment of Adult Literacy (NAAL).” AMA Foundation. Available at www.ama-assn.org/resources/doc/ama-foundation/hl_report_2008.pdf.
Williams, Mark V., David W. Baker, Ruth M. Parker, and Joanne R. Nurss. 1998. “Relationship of Functional Health Literacy to Patients' Knowledge of Their Chronic Disease: A Study of Patients with Hypertension and Diabetes.” Archives of Internal Medicine, 158:2, 166–172.
Xu, Lisa, and Zia Bilal. 2012. Financial Literacy around the World: An Overview of the Evidence with Practical Suggestions for the Way Forward. World Bank Policy Research Working Paper No. 6107. Available at http://ssrn.com/abstract=2094887.
Yates, Dan, and Chris Ward. 2012. “Are Your Personal Financial Characteristics Healthy?” Journal of Business & Economics Research 10:4, 225−232.
Zajonc, Robert B. 1980. “Feeling and Thinking: Preferences Need No Inferences.” American Psychologist 35:2, 151–175.
ABOUT THE AUTHORS
Talya Miron-Shatz is Founding Director of the Center for Medical Decision Making, Ono Academic College, and CEO of CureMyWay, a start-up company that creates software to support patients' decision making and healthy habit formation. She was a post-doctoral research fellow at Princeton University, and taught consumer behavior at the Wharton Business School, University of Pennsylvania. She examines how patients and health care professionals understand and convey risk information, and what makes people follow warnings and lifestyle regimens. Her research is widely published in peer reviewed journals including Psychological Science, Health Psychology, and Emotion. As part of her mission of translating academic knowledge into action, she consults pharmaceutical companies and related agencies, and writes about medical decision making for Psychology Today. Dr. Miron-Shatz received an MA in psychology and communications and a PhD in psychology from The Hebrew University.
Stephanie Gati is a recent graduate from Princeton University, with a degree in Ecology and Evolutionary Biology and a certificate in Global Health and Health Policy. Ms. Gati is a Fellow in the Princeton University Project 55 program at Aeras Global TB Vaccine Foundation in Rockville, Maryland. She is supporting teams performing clinical trials of six tuberculosis vaccine candidates in various African countries. She became interested in vaccine development after conducting her Princeton University senior thesis research on malnutrition and pneumococcal conjugate vaccine efficacy in rural populations in Kenya. During the summer of 2011, Ms. Gati was a Global Health Intern Johnson and Johnson in the Department of Government Affairs, working on initiatives to promote chronic disease prevention. Ms. Gati plans to attend medical school and become a public health physician.
ACKNOWLEDGMENT
The authors thank Glen Doniger and Joshua Zuckerman for their insightful contributions.