
Chapter 19
Health Aspects of the Hebei Spirit Oil Spill
Abstract
The oil spill that occurred in Taean on December 7, 2007, was the largest oil spill ever in Korean waters. This accident took place close to residential areas, and as a result, it affected the physical and psychological health of the residents. An extensive health survey was conducted on local residents, volunteers, and military personnel immediately after the accident. The results showed that the oil spill increased the physical symptom prevalence, depression, suicidal impulse and psycho-social stress of residents. Consequently, a long-term follow-up survey on the health of local residents was suggested, and in response, the Korean Ministry of Environment (MOE) designated Taean Environmental Health Center (TEHC) as the agency in-charge for the task and ordered a medium-to long-term health survey. TEHC is monitoring the adults and children in the oil spill disaster area. In addition, the center is also engaged in studying prevention and the health effects of the oil spill, establishing a biospecimen bank and database, providing medical services and health consultations, providing education and health promotion programs, and alerting the international community on the study of health effects from oil contamination. Since the first survey in 2009, health surveys of adults and children have been conducted biennially, and as of February 2016, a total of approximately 16,000 people (approximately 12,460 adults and 3580 children) had participated in the surveys. In addition to this, a survey is also being conducted on the health effects of the oil spill on pregnant women and infants. The health survey included questionnaires, health examinations, and specialized tests, which were used to assess how health status is affected by oil spill exposure levels. This was performed by analyzing the concentrations of heavy metals, volatile organic compounds, and polycyclic aromatic hydrocarbons, along with oxidative damage index through biomarkers. Health education, laughter therapy, nutrition education, and prescribed exercise are being conducted for adults, while “Health Nanuri (sharing) Camp” is being conducted for children. Along with the continued health monitoring of Taean residents, future plans include concentrated efforts in the area of follow-up surveys of volunteers who participated in the cleanup activities at the initial stage of the accident, mechanistic studies on the health effects of oil exposure through toxicology and genetic studies, in-depth studies linked to other ecotoxicological studies, sharing of health study results through international cooperation, and expert training.
Keywords
Biomarkers; Health effects; Hebei Spirit; Long-term health survey; Oil spill
19.1. Introduction
19.1.1. Background
Around 7 a.m. on December 7, 2007, at a location 5 miles northwest off the coast of Mallipo in Taean-gun (county), Chungcheongnam-do (South Chungcheong Province) in the Republic of Korea (latitude 36° 52′00″, longitude 126° 02′09″), a floating crane belonging to Samsung Heavy Industries collided with the oil tanker Hebei Spirit which was anchored at the time to avoid the winter storm (Fig. 19.1).
From this accident, approximately 12,547 kL (∼10,900 t) of crude oil spilled onto the waters off Taean (Fig. 19.2) [1]. This accident was the largest oil spill ever in Korean waters with the oil spillage exceeding the total 10,234 kL of oil spilled in marine pollution accidents between 1997 and 2006. This accident caused pollution to a total of roughly 1052 km of seashore of the North Jeolla and South Chungcheong Province, which includes Taean Coast National Park, also causing serious damage to 3000 ha of fisheries, aquafarms, and swimming beaches (Fig. 19.3).
Taean-gun was the region most affected by this accident and the 63,939 residents of two towns and six townships within Taean-gun lost their primary means of livelihood, in the form of aquafarming, fishing, and tourism (as of 2007) [2]. From the time of the accident to July 4, 2008, the cumulative total number of people who participated in the land-based cleanup activities was 2,122,296, which included 556,343 residents, 1,226,730 volunteers, 152,695 military personnel, 32,356 police, 17,394 coast guard, 6663 members of the Korea Marine Environment Management Corporation, 53,431 corporate employees, and 76,684 members of various local authorities (Table 19.1) [1].

The residents participated in the cleanup activities starting from the day after the accident, December 8th, while volunteers started participating 2 days after the accident, December 9th. During the initial stage of the cleanup activities, work was performed without any protective gear such as protective clothing, protective gloves, or masks. As such, the workers were exposed to the crude oil through the respiratory tract and skin.


19.1.2. Toxicity and Health Effects of the Oil Spill
The crude oil that Hebei Spirit was carrying included three types of oils from three different sources: Iran, Kuwait, and United Arab Emirates. The contents of crude oil include volatile organic compounds (VOCs), polycyclic aromatic hydrocarbons (PAHs), and heavy metals [3]. The hazardous chemicals contained in crude oil can not only cause the destruction of ecosystems, but can also have direct and indirect effects on health. Moreover, they can also cause secondary social issues from economic losses and the destruction of communities. In particular, such health issues can lead to not only physical illnesses, but also to mental illnesses, such as anxiety disorders, depression, and posttraumatic stress disorder (PTSD).
Table 19.1
Number of Cleanup Work Participants in Hebei Spirit Oil Spill, 2007, Taean, Korea (as of July 4, 2008)
| Participants | Summation of Daily Participants (%) |
| Residents | 5,56,343 (26.2) |
| Volunteers | 12,26,730 (57.8) |
| Military personals | 1,52,695 (7.2) |
| Public officers | 76,684 (3.6) |
| Others | 2,49,884 (11.8) |
| Total | 21,22,296 (100.0) |
From Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.
19.1.2.1. Volatile Organic Compounds
VOCs evaporate easily into the atmosphere due to their high vapor pressure, and depending on the substance, they can be carcinogenic to the human body as well. Benzene, toluene, ethylbenzene, and xylene are the best known VOCs. When exposed to low concentrations of benzene, light symptoms such as drowsiness and dizziness may appear, whereas vomiting, convulsions, and even coma can be brought on from exposure to high concentrations of benzene. Exposure to toluene can cause headaches and memory loss, while repeated exposure to high concentrations can even produce speech impairment, vision loss, hearing loss, as well as kidney damage. Exposure to high concentrations of ethylbenzene can cause vertigo, along with eye and throat irritation. Moreover, continued exposure to low concentrations may cause kidney damage as well. Short-term exposure to high concentrations of xylene can lead to irritation in the eyes, nose, throat, and skin, as well as breathing difficulties and damages to the lungs, liver, and kidneys.
19.1.2.2. Polycyclic Aromatic Hydrocarbons
PAHs, among which some are carcinogens, are generated from thermal decomposition or incomplete combustion of oil and are easily absorbed usually through the respiratory tract. Many substances with five to six benzene rings show carcinogenicity, and damage red blood cells and reduce the red blood cell count. The International Agency for Research on Cancer (IARC) has classified naphthalene as a Group 2 human carcinogen. Short-term exposure to anthracene can damage the skin and cause burning or itching, headaches, gastritis, and enteritis.
19.1.2.3. Heavy Metals
Crude oil contains heavy metals, such as mercury, lead, and cadmium. Mercury is absorbed into the body by respiration or from food, and exposure to highly concentrated mercury vapors can irritate the airway mucosa and cause acute pneumonia accompanied by fever and respiratory problems. Such exposure can also induce chronic symptoms in the form of neurologic and mental disorders, such as agitation and anxiety, depression, and memory decline. Moreover, exposure to mercury during infancy or adolescence is known to affect physical growth and development, as well as the development of the immune and neural systems.
Lead is absorbed from food, paints containing lead, or contaminated water, and exposure to lead can lead to neurodevelopmental disorders in children [4]. Recent studies have shown that even exposure to very low concentrations of lead can cause neurobehavioral developmental disorders, such as learning disorders, hyperactivity disorder, and IQ decrease in children. This demonstrates that lead toxicity does not have a threshold, and has resulted in a growing trend of reinforcing management of such toxic substances.
Cadmium is introduced in the body mostly through food and is known to affect the kidneys, skeletal system, lungs, and reproductive system. Moreover, it is known to affect the IQ of children, as well as cause mental retardation and attention deficit disorders.
19.2. Acute Health Effects
19.2.1. United Committee for Investigation of Acute Health Problems for the HS Oil Spill
After the accident, the “United Committee for Investigation of Acute Health Problems for the HS Oil Spill” (UCHS) was created, which comprised environmental citizen groups, academicians, experts, and government agencies. In the initial stage of the accident, independent environmental exposure and health surveys were conducted by academic and citizen groups owing to an absence of a unified agency. UCHS conducted, in a unified manner, biological sampling and surveys that were being conducted independently by various agencies and groups. Furthermore, it also oversaw joint discussions on the direction of health assessments, survey methods, and the publishing of survey results.
19.2.2. Assessment of Acute Ambient Exposure
Because a systematic study on ambient exposure was not performed after the accident, data on air quality and hazardous agent concentration measurements taken by various agencies were collected and used to estimate their atmospheric concentrations in the contaminated region immediately after the accident. This was accomplished through a computer simulation process via a geographical information system (GIS) technique and modeling [5]. Modeling results indicated that all benzene, which is highly volatile, evaporated within 10 h of the accident, while toluene, ethylbenzene, and xylene evaporated within 48 h. Other VOCs mostly evaporated within 4 days. In terms of 16 PAHs, most of the naphthalene evaporated within 15 days, while the evaporation of acenaphthylene, acenaphthene, and fluorene required approximately 1 month, and other PAHs continued to evaporate over a period of 2 months or longer (Fig. 19.4).

Figure 19.4 Evaporation rate of spilled oil with time: (A) representative toxic volatile organic compounds; (B) light components crude oil, in Hebei Spirit oil spill, 2007, Taean, Korea. From Kim JH, Kwak BK, Ha M, Cheong HK, Yi J. Modeling human exposure levels to airborne volatile organic compounds by the Hebei Spirit oil spill. Environmental Health and Toxicology 2012;27:e2012008.
Calculated results of acute exposure to VOCs and PAHs from air dispersion modeling showed high concentrations in the coastal areas close to the accident site, which indicated that residents of these coastal areas and people who performed cleanup activities near the coast were exposed to high concentrations of VOCs and PAHs in the first 5 days.
19.2.3. Urinary Biomarkers Assay
Between 2 and 8 weeks after the accident, urine samples were collected on three occasions from the residents, children, pregnant women, and volunteers. The subjects were selected from those who completed the questionnaire without any missing answers and those who were surveyed repeatedly to allow periodic changes to be observed. The control group was selected from those who were deemed appropriate from the control regions. Samples were collected from a total of 288 residents and children 2–3 weeks after the accident in the first survey; a total of 30 residents 5–6 weeks after the accident in the second survey; and a total of 188 people, including 66 residents and 43 children who were followed up with repeatedly and 79 newly pregnant women, 8 weeks after the accident in the third survey.
Concentrations of four types of urinary VOC metabolites (t,t-muconic acid, mandelic acid, hippuric acid, and methylhippuric acid), two types of PAH metabolites (1-hydroxypyrene and 2-naphthol), and five types of heavy metals (lead, mercury, cadmium, manganese, and nickel) were analyzed from the selected subjects. The residents who participated in the cleanup activities showed higher lead, mercury, and cadmium concentrations than the residents from the control region, while nickel and manganese showed little difference [6].
Analysis of VOC metabolites concentrations within the body, adjusted for gender and age, showed no significant difference between the contaminated and control regions. Although mandelic acid concentrations were higher in those who participated in the cleanup activities than the control group, the difference was not statistically significant. Among those who participated in the cleanup activities, their mandelic acid concentrations measured at 5–6 weeks after the accident were significantly higher than the concentrations measured 2–3 weeks after the accident. The concentration of the two types of PAH metabolites also did not show a significant difference between the residents who participated in the cleanup and the control group. Follow-up surveys of the participants of the cleanup activities showed that concentrations of both 2-naphthol and 1-hydroxypyrene were significantly higher between 2 and 3 weeks than between 5 and 6 weeks after the accident. Children and pregnant women did not show significant differences between the contaminated and control regions with respect to concentrations of VOCs and PAHs [1]. Comparisons of biological exposure to VOC metabolites in the volunteers from before and after participating in cleanup activities showed significantly higher t,t-muconic acid and mandelic acid concentrations after the cleanup. Among PAH metabolites, the concentration of 1-hydoroxypyrene was significantly higher [7].
19.2.4. Health Effects
A health survey was conducted on 3003 persons including the residents, volunteers, pregnant women, children, and infants. The questionnaire surveys were conducted on three occasions. The first survey included data from approximately 1509 people collected from on-site surveys that were conducted independently by citizen groups and relevant agencies 2–6 weeks after the accident. The second survey was a repeated, follow-up survey on 79 residents and 233 children, and was conducted 8 weeks after the accident. The third survey was conducted on 1225 children, 80 pregnant women, and 189 infants and toddlers 4–5 months after the accident. The residents and volunteers were surveyed on-site, while the children were surveyed at school under the supervision of their teachers. The mothers, infants, and toddlers were surveyed via personal interviews by visiting their homes. Subjective physical symptoms and mental health were assessed through the questionnaire survey.
19.2.4.1. Physical Symptoms
19.2.4.1.1. Residents
A questionnaire survey on subjective physical symptoms was conducted on residents who participated in the cleanup activities for at least 1 day, on all residents living close to the accident site (20 km southeast and 24 km east), and on residents of islands relatively far from the site (65 km).
Questions on protective gear included the use of gloves (97.9%), rubber boots (94.4%), masks (71.3%), filter masks (39.3%), and caps (65.5%). With respect to how much oil had got on their skin, 37.8% of the respondents replied “much or very much.”
A total of 41 questions, divided into 14 symptom groups, were surveyed about subjective physical symptoms. In all 14 symptom groups of subjective physical symptoms, ≥50% of the residents responded as having at least one symptom and the complaint rate for most of the symptoms decreased over time, whereas symptoms of the nose, throat, trachea, and skin, along with headaches, nausea, vomiting, palpitations, and musculoskeletal symptoms actually increased after 6–8 weeks (Fig. 19.5). Reports of physical symptoms increased in those who participated in the cleanup activities for longer and had greater skin exposure to oil (Figs. 19.6 and 19.7).

Figure 19.5 Prevalence of subjective physical symptom by time among residents participating in cleanup work in Hebei Spirit oil spill, 2007, Taean, Korea. Drawn based on Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.

Figure 19.6 Prevalence of subjective physical symptoms based on the increasing days of cleanup work at the time of 2–8 weeks after the accident of Hebei Spirit oil spill, 2007, Taean, Korea. Drawn based on Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.

Figure 19.7 Prevalence of subjective physical symptoms based on the increasing degree of skin contamination by crude oil at the time of 2–8 weeks after the accident of Hebei Spirit oil spill, 2007, Taean, Korea. Drawn based on Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.
An analysis of 154 people who participated in the cleanup activities showed that those with hippuric acid levels higher than the median experienced 2.97 times higher incidence of nasal irritation and 3.01 times higher incidence of nausea and vomiting sensations. Moreover, those with methyl-hippuric acid levels higher than the median reported 4.38 times higher incidence of fatigue and fever than those below the median. Meanwhile, the subjects who showed high 1-hydroxypyrene concentration levels reported 4.16 times higher incidence of musculoskeletal symptoms than those with lower concentrations. Eye and skin irritation symptoms appeared higher by 20 and 5 times, respectively, in the subjects with high urinary lead concentrations. Moreover, the subjects with high urinary mercury concentrations had a complaint rate of irritation symptoms 5 times higher than those without. The subjects with high urinary nickel and cadmium levels had skin irritation symptoms that were 2 times higher, while headaches and palpitations were 4 times higher (Fig. 19.8) [6].
19.2.4.1.2. Children
19.2.4.1.3. Pregnant Women
Subjective physical symptoms of pregnant women residing in the Taean region were surveyed via a questionnaire at 2 months after the accident. Due to a lack of monitoring data from the initial stage of the accident, amount of exposure to benzene, toluene, ethylbenzene, o-xylene, and m,p-xylene was calculated through modeling.
After the oil spill, the complaint rate of headaches was significantly higher in those whose place of residence was closer to the contamination site, while the group that had ever went out to beach showed a higher complaint rate of skin irritation, abdominal symptoms, and muscle aches than the group that stayed home. Analyses of correlations between the distance between place of residence and atmospheric VOC concentrations, and complaint rate of subjective physical symptoms showed that mothers who resided in the areas with high benzene concentrations had a significantly higher complaint rate of nausea, vomiting, and memory and cognitive symptoms. Pregnant women who resided in the areas with high toluene concentrations on the day of the accident had a significantly higher complaint rate of skin irritation than pregnant women residing in areas with low concentrations. Pregnant women who resided in areas with high atmospheric cumulative concentrations of ethylbenzene, o-xylene, and m,p-xylene had a significantly higher complaint rate of abdominal pain than pregnant women residing in areas with lower concentrations [8].

Figure 19.8 Risk of physical symptoms based on the level of urinary VOCs and PAHs metabolites and metals in urine obtained at the time of 2–6 weeks after the accident, in 154 residents participating in cleanup of the Hebei Spirit oil spill, 2007, Taean, Korea. From Cheong HK, Ha M, Lee JS, Kwon H, Ha EH, et al. Hebei Spirit oil spill exposure and subjective symptoms in residents participating in clean-up activities. Environmental Health and Toxicology 2011;26:e2011007.

Figure 19.9 Risk of symptoms based on the distance from the residential house to the nearest contaminated coastline at the time of 3–8 weeks after the accident of Hebei Spirit oil spill, 2007, Taean, Korea. Drawn based on Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.

Figure 19.10 The risk of symptoms based on the distance from the school to the nearest contaminated coastline at the time of 3–8 weeks after the accident Hebei Spirit oil spill, 2007, Taean, Korea. Drawn based on Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.
19.2.4.1.4. Volunteer
A survey of subjective physical symptoms in 565 volunteers through a questionnaire given 2–3 weeks after the accident showed that eye and mucosal irritations were the most common complaints with 46.9% and 41.6%, respectively, and headache (42.0%), fatigue and fever sensation (37.4%), and musculoskeletal symptoms (35.8%) also showed a high complaint rate. Compared to volunteers who participated in the cleanup activities for 1 day, those who participated for 2 days or longer had a significantly higher rate of visual disturbance, palpitation, fatigue and fever sensation, memory and cognitive disturbance, abdominal pain, nasal and bronchus irritation, and headaches [7].
19.2.4.2. Psychological Health
19.2.4.2.1. Residents
A mental health assessment was conducted on 288 residents of the contamination site 2–6 weeks after the accident, and on 79 of these same residents 8 weeks after the accident via follow-up survey. A mental health assessment was conducted using three different questionnaires: Psychosocial well-being index (PWI), the Center for Epidemiologic Studies Depression Scale (CES-D), and questions developed for suicidal ideation.
Psychosocial stress level in residents of the contamination site was 1.2–4 times higher than in the general workers for all age groups (Fig. 19.11). Prevalence of depression was higher by 1.2–4 times in all age groups, as compared to the general public or general workers in Korea (Fig. 19.12). Suicidal ideation of the residents was 22.4%, which was higher than the 18.4% reported from a national sample in Korea in 2005, and in particular, this percentage was 2.8 times higher in those in their 40s (Fig. 19.13). For psychosocial analysis based on the distance from the contamination site, distances were divided into four groups: <15 km, 15–25 km, >25 km from the contamination site, and the inland region virtually unaffected by the oil spill. The posttraumatic diagnostic scale (PDS) was used to diagnose PTSD; CES-D was used to measure depression; the Korean version of the scale for suicidal ideation was used to measure suicidal ideation; and the Korean version of the symptom checklist-90-revision (SCL-90-R) was used to measure anxiety.
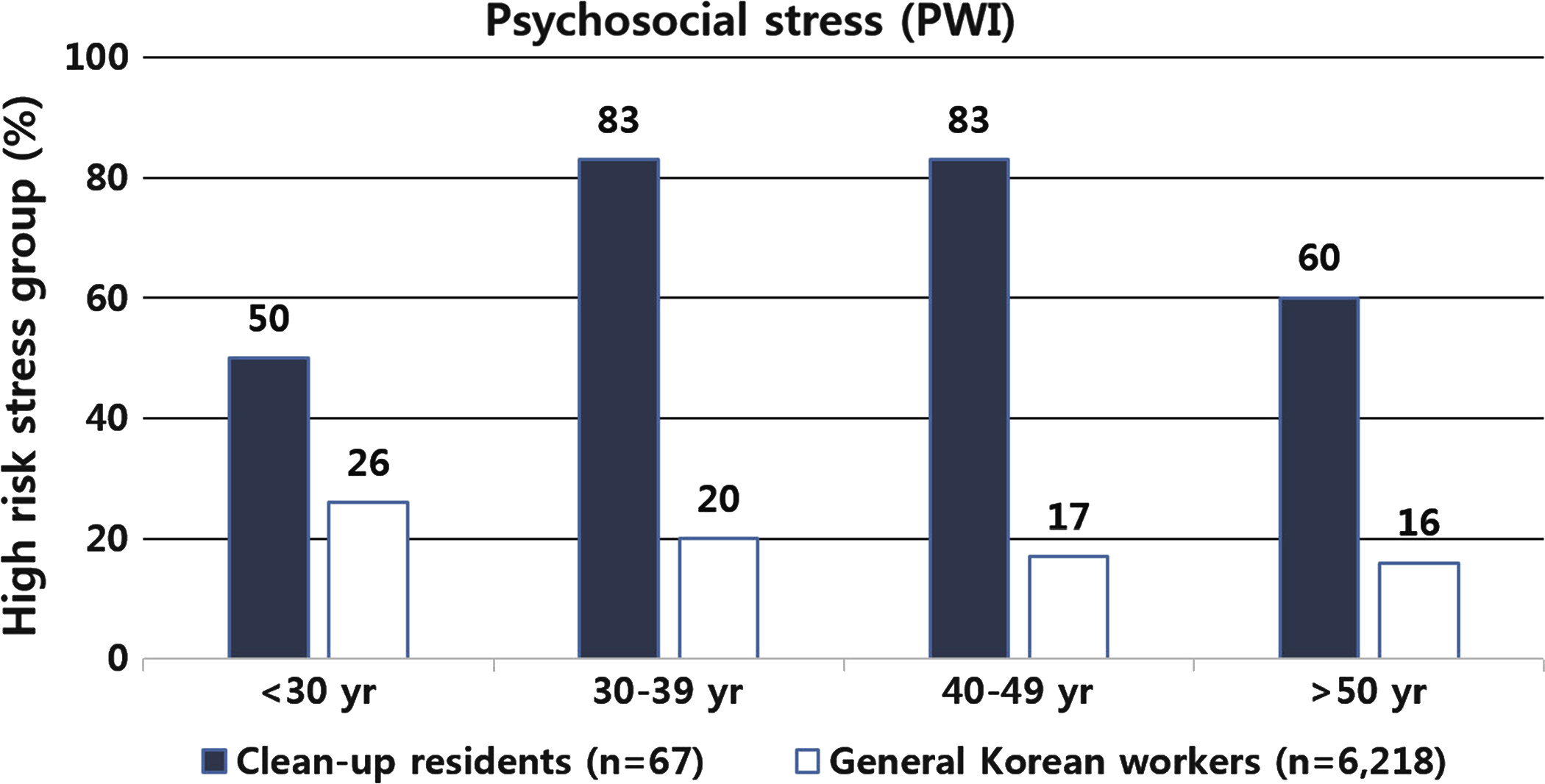
Figure 19.11 Psychosocial stress measured by PWI (Psychosocial Well-being Index) among residents participated in cleanup work at the time of 3–8 weeks after the accident of Hebei Spirit oil spill, 2007, Taean, Korea. Drawn based on Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.

Figure 19.12 Depression measured by CES-D (Center for Epidemiological Studies-Depression) in residents participated in cleanup work at the time of 3–8 weeks after the accident of Hebei Spirit oil spill, 2007, Taean, Korea. Drawn based on Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.

Figure 19.13 Prevalence of suicidal impulse in residents participated in cleanup work at the time of 3–8 weeks after the accident of Hebei Spirit oil spill, 2007, Taean, Korea. Drawn based on Ministry of Environment. Investigation of acute health problems among people exposed to the Hebei Spirit oil spill. Ministry of Environment; 2008.
Among all subjects, PTSD, depression, suicidal ideation, and anxiety symptoms were found in 19.5%, 22.0%, 2.3%, and 4.2% of the subjects, respectively. PTSD, depression, suicidal ideation, and anxiety symptoms were higher in the areas within close range to the oil spill, and all of the values appeared high in occupational groups with relevant work, such as fishing and tourism. The results of mutually adjusted analysis of the distance from the contamination site and occupation showed that post traumatic stress (PTS) and depression were significantly influenced by both distance and occupation, whereas suicidal ideation and anxiety were influenced more strongly by occupation than distance [9].
19.2.4.2.2. Children
Mental health questionnaire surveys were conducted on a total of 1361 children from 13 primary schools in the Taean region; the first survey was done 8 weeks after the accident and the second survey was 5 months after the accident. The distance from the contamination site to their residence or school was measured using GIS. Depression was assessed using the Korean version of the children's depression inventory, while anxiety was assessed using Korean version of the state-trait anxiety inventory for children (SAIC, TAIC).
Prevalence of depression in children from the exposed region was 15.3% after 8 weeks of the accident and 9.9% after 5 months of the accident, while prevalence of anxiety was 12.7% after 5 months of the accident. These values were more than twice the values found in children of similar age who resided in similar cities.
Children attending a school with a distance from the contamination site ≤1.6 km were at 2.2 times higher risk of depression than children with a distance ≥3.7 km. Shorter distances from the contamination site to school resulted in a significant increase in the risk of depression. However, there was no significant difference with respect to the distance to their residence. Although the risk of anxiety was higher in those whose home or school was closer to the contamination site, the difference was not significant [10].
19.2.5. Summary
A summary of acute health effects is as follows:
1. Estimation of initial VOCs and PAHs exposure conducted through air dispersion modeling indicated high concentrations of VOCs and PAHs in coastal areas close to the accident site in the first few days after the accident. Therefore, it is suspected that the residents who live in these coastal areas and the people who participated in the cleanup activities in these areas were highly exposed to VOCs and PAHs in the initial stage.
2. The biological sample testing on the residents showed that mandelic acid concentrations measured 5–6 weeks after the accident were significantly higher than the concentrations measured 2–3 weeks after the accident while PAH metabolites, 2-naphthol, and 1-hydroxypyrene concentrations measured 2–3 weeks after the accident were significantly higher than the concentrations measured 5–6 weeks after the accident. The residents who participated in the cleanup activities showed higher concentrations of lead, mercury, and cadmium than those in the control region, and thus, follow-up monitoring was deemed necessary. Analysis of urine samples from the volunteers taken before and after the cleanup activities showed that t,t-muconic acid, mandelic acid, and 1-hydoroxypyrene were significantly higher after the cleanup than before.
3. The subjective physical symptoms in the residents and volunteers who participated in the cleanup activities showed an increased complaint rate when the number of days involved in cleanup activities were higher, protective gear was not worn, and amount of exposure to oil during the work was also higher. Moreover, complaint of subjective physical symptoms also increased in children from the exposed region, when the children lived or went to school in areas close to the contaminated coast.
4. The levels of depression and psychosocial stress in the residents who participated in the cleanup activities were higher than those of general workers. PTS and depression were found to be significantly affected by the distance from the contamination site and occupation. Children who attended schools in areas close to the contamination site showed higher risk of depression.
In conclusion, the Hebei Spirit oil spill was found to influence the physical and mental health of the residents, volunteers, children, and pregnant women, and such findings suggest a need for consistent health promotion programs and health effect assessments on the residents and children through future medium-to long-term follow-up surveys.
19.3. Long-Term Health Effects
19.3.1. Taean Environmental Health Center
Based on the results of acute health effects surveys, the need for a systematic and stable research agency for creating consistent programs for promoting the physical and mental health of the residents and conducting medium-to long-term health effect assessments related to the crude oil spill was suggested. In an effort to address such a need, the Taean Environmental Health Center (TEHC) was established in August of 2008, on the basis of the Framework Act on Environmental Policy and Environmental Health Act. The TEHC is designated by the Ministry of Environment (MOE) and has received financial support from the MOE and local governments, the Taean-gun and Chungcheongnam province.
The TEHC has been conducting the oil spill contamination–related health surveys, monitoring residents and children on an annual basis, and is also conducting research on health effects. In particular, the center has established a biobank of blood, urine, and hair samples collected from the annual health surveys, as well as a database of approximately 14,000 persons from the past 8 years.
In addition, the center has been also providing environmental disease–related information and prevention guidelines for health promotion of the residents, and also conducting “Environmental Diseases Camp” for children and “Health Promotion in Daily Life Program” for adults, which include prescribed exercise program, laughter therapy, and mental health consultation.
19.3.2. Hypotheses
Crude oil spills can affect human health via various routes, including introduction through breathing, contact with the skin, and from the atmosphere, ocean, and soil. Because VOCs and some of the PAHs contained in crude oil are highly volatile, they pose the greatest threat during the period from when the accident occurs until 1 week after, and residents who participate in the cleanup activities during this period or live near the accident site are exposed to hazardous substances through inhalation. In the case of the Taean oil spill, because of a lack of awareness about the health effects from crude oil and proper guidelines in the initial stage of the accident, cleanup activities were started without having protective gear, such as protective clothing and masks, ready for use. It is suspected that as a result of this, the risk of exposure to hazardous substance through breathing may have been high.
Furthermore, when people participate in the cleanup activities without proper protective gear, crude oil can come in contact with the skin. When this happens, the skin can become itchy or turn red similar to a burn injury. Even without such direct exposure from breathing or absorption through the skin, contaminants that are introduced to the sea, air, and soil can contaminate agricultural and fishery products and have an indirect effect on the health of humans who consume such products. Fetuses can be exposed indirectly through the placenta of mothers who were exposed.
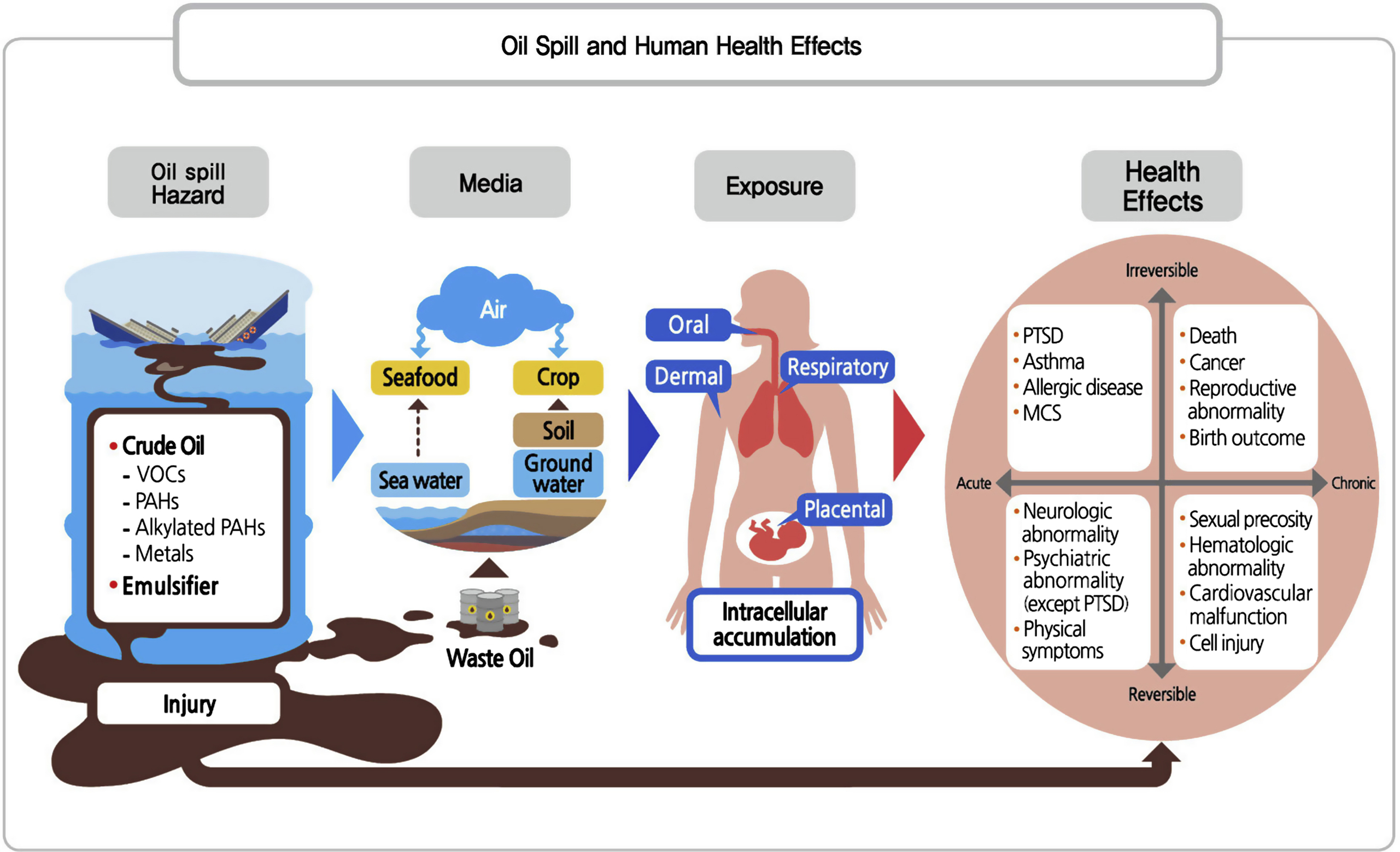
Hazardous substances that enter the body in this manner can have acute and long-term effects on a person's nervous, hematopoietic, respiratory, cardiovascular, and immune systems, and can affect the birth, growth, and development of a fetus. Moreover, it can be divided into four types depending on the onset of the disease and the efficiency of recovery. The cases can be further divided into those in which health effects occur in the early stage of the accident and whether they persist for a long time, or are recovered relatively easily over time. In contrast, there are other cases in which no signs are seen in the early stage of the accident, but health effects begin to appear several months or years later and whether those persist throughout one's lifetime, or are recovered or diluted from physical growth or aging (Fig. 19.14) [11].
19.3.3. Overview of Long-Term Health Survey
The purposes of the medium- to long-term health surveys were to assess the level of human exposure to contaminants in the spilled oil following the Hebei Spirit oil spill and the health status of residents in the oil-damaged area after the accident. The survey also aimed to analyze the correlations between exposure and health status in an effort to provide scientific and objective data for damage restoration and health promotion for the residents. In order to achieve this, the goal was to establish cohorts and conduct medium-to long-term follow-up surveys.
After the first survey in 2009, follow-up surveys are being conducted biennially on adults, children, and adolescents. The survey in 2009 was conducted on 9246 adults and 1172 children and adolescents, and since then, biennial follow-up surveys are being conducted on approximately 800 to 1200 people (Table 19.2). The surveys include questionnaires, health examinations, and biomarker analyses using urine and blood samples. The surveys are conducted after a review process through the institutional review board.
19.3.3.1. Questionnaires
The questionnaires were in a self-reporting format by default. The questionnaires for the elderly were completed via interviews by trained surveyors, while the questionnaires for children and adolescents were completed by their parents or guardians. The questionnaires obtained information on sociodemographic characteristics (occupation, education, economic status, etc.), lifestyle habits (drinking, smoking, exercise, etc.), residential environment, history of exposure to oil contamination (participation in cleanup, whether protective gear was worn during cleanup, number of days participating in cleanup, etc.), history of exposure to atmospheric contaminants and electromagnetic waves, dietary habits, disease history. Mental health status (depression, PTSD, anger, unstable character and condition, etc.) was assessed mostly using the existing scales of the Korean version.
19.3.3.2. Health Examination
Health examinations were performed inside the examination room at the Taean Medical Center and the specialized examinations included blood tests, urine tests, anthropometric measurements, blood pressure, general examination, lung function test, heart rate, blood aging test, and allergy skin prick test.

19.3.3.3. Biomarker Measurements
Heavy metals (lead, mercury, cadmium), oxidative damage index (malondialdehyde (MDA), 8-OHdG), gene mutation test, and epigenetic studies were performed using blood and urine samples.
19.3.3.4. Biorepository
Urine and blood collected were frozen and stored for analyses, and the original documents, including the questionnaires, were kept in a warehouse.
19.3.3.5. Exposure Classification of the Study Site
Coastal residents who faced coasts contaminated with a thick layer of oil in the initial stage of the accident were considered to be highly exposed, and as such, they were classified as being in the cleanup area (high-exposure area), while the other areas were classified as the affected area (low-exposure area). The exposure distance was derived by calculating the distances from the accident site to the residences and schools using the GIS.
19.3.4. First Long-Term Health Survey
The first medium- to long-term health survey was conducted between January 2009 and June 2010. The survey had four goals: environmental exposure assessment, biomarkers assessment, physical health assessment, and mental health assessment and providing mental health programs [12].
19.3.4.1. Assessment of the Environmental Exposure
The assessment of environmental exposure caused by the oil spill included measurements of concentrations of hazardous substances in the oil from living and natural environments, a survey of dietary habits of Taean residents, and an assessment of the amount of exposure Taean residents had to hazardous substances in the oil. In addition, exposure levels by periods were measured by estimating the concentrations of hazardous substances in oil remaining in the atmosphere via computer simulation on the participants of the cleanup activities, residents, and visitors.
19.3.4.1.1. Assessment of Exposure Level to Hazardous Components in Oil
Among the residents of Taean who were directly affected by the oil spill, exposure assessment was conducted on 30 children and 30 adults who participated in the cleanup activities and received a health examination. Samples for exposure assessment included food consumed from three daily meals, seafood consumption, dust from the floor of homes of the survey subjects, soil around the residence and school, and wipe sample from the soles of the foot contacting the beach as living environmental samples. For natural environmental samples, the groundwater and air were collected, and soil near schools and seafood caught near Taean were obtained.
First, PAH analysis found that ∑15 PAH concentrations in the food consumed by the subjects was 0.36–5.13 ng/g, which was similar or lower than the results from previous studies and also lower than the concentration values from other regions. ∑15 PAH concentrations in seafood were 0.42–42.63 ng/g, with mussels showing the highest values among shellfish and flounder showing the highest concentrations among fish. With respect to the seafood samples, their concentrations were higher than those of other foods, but they were not much different from or even lower than the concentrations analyzed in seafood collected from Taean over a set period of time, starting from when the oil spill occurred.
Dust samples from the floor of homes were collected using gauzes and vacuum collectors. Analysis of dust collected using gauze applied with alcohol showed that ∑15 PAH concentrations were ≥13 times higher than those measured in other regions. Meanwhile, ∑ TEQ PAH concentrations were at least 17 times higher than Seoul or other farming regions. Soil samples from living areas of the subjects showed ∑15 PAH geometric mean value of 9.85 ng/g, which were at least 11 times lower than the concentrations from roadsides in Seoul or industrial areas, and 7 times lower in comparison with same residential areas. ∑15 PAH concentrations in air (PM10) were 0.16–6.20 ng/m3, which were similar to levels before the oil accident and actually lower than other regions. The concentration range of groundwater collected from five locations around Taean was below the recommended value for drinking water.
An assessment of personal exposure to PAHs and metal elements in 60 Taean residents showed no difference in the levels of exposure to most metal elements between children and adults, whereas cadmium was approximately two times higher in adults (0.20 μg/kg/day) than in children (0.10 μg/kg/day), and lead was approximately three times higher in children (0.33 μg/kg/day) than in adults (0.13 μg/kg/day).
19.3.4.1.2. Change of Dietary Habits and Food Safety Assessment in Residents
A focus group interview was conducted on 50 people who reside close to the oil spill accident site to examine changes in their health, economic changes in their family, dietary changes, changes in food purchasing and cooking, and future food purchasing plans. The interview results showed that the subjects complained of dizziness, vomiting, diminished vision, skin diseases, loss of appetite, and insomnia after participating in the cleanup activities. Economically, people involved in fishery without gear complained of the greatest economic damage, while those involved in fishery, tourism, and seafood sales were also found to have suffered significant economic damage. With respect to dietary changes, people employed in fishery, who suffered the greatest economic damage, responded that their consumption of all foods, including seafood and meat, decreased due to reduced income which made food purchasing difficult [13].
Among those who participated in health examinations in the Taean region, 808 people who provided information of their food and nutrient consumption via the food frequency questionnaire were divided into three groups: government employees, the cleanup area residents (high-exposure area), and the affected area residents (low-exposure area). Analysis of their food and nutrient consumption showed that the average daily calorie intake was significantly lower in the cleanup area residents (1584 kcal), as compared to the affected area residents (1781 kcal) and government employees (1946 kcal). Even after adjusting for age and gender, consumption of calories, fat, and carbohydrates, except proteins, was significantly lower in the cleanup area residents, and consumptions of folic acid and vitamins B1, B6, and E were also significantly lower than the other two groups. Nutrient consumption levels of those being surveyed were compared to dietary reference intakes for Koreans [14] for analysis of the percentage of subjects consuming below the recommended level. As a result, the percentage of those who were consuming below the estimated energy requirements was significantly higher in the cleanup area residents (77.9%), as compared to the affected area residents (66.2%) and government employees (69.5%). Although consumption of proteins and iron was good, the percentage of those consuming below the average requirements for folic acid, calcium, riboflavin, thiamine, and vitamin C was ≥45% of the survey subjects.
These study results indicated that the economic damages and cleanup activities following the oil spill affected not only the health of the residents, but also affected their dietary habits, which led to a decrease in food consumption. Moreover, dietary habit surveys found that the nutrient consumption status of the residents showed that consumption of various nutrients, including calories, was significantly lacking.
19.3.4.1.3. Environmental Exposure Modeling Through Computer Simulation
Assessment of the level of bodily exposure to crude oil components in the initial stage of the accident is necessary for assessing their health effects on the residents in the contaminated area. Because actual measured values from the initial stage of the Hebei Spirit oil spill were lacking, a modeling technique was used to make a comprehensive assessment of the level of bodily exposure. In addition to the acute ambient exposure modeling, a comprehensive computer simulation was performed repeatedly with an extension of the target periods.
Focusing on the area near the accident site and the western Sea, concentrations of crude oil components were calculated, and the expansion, distribution, and transport processes of the spilled crude oil components in the sea and air were comprehensively tracked to calculate the atmospheric and marine concentrations of crude oil components. Based on actual measured data from aerial photo analysis and satellite images, expansion of the oil spill in the ocean was assumed to be the source of distribution for the crude oil components and calculations were made accordingly. The duration of the computer simulation was set to 1 year from the accident. Modeling was linked to the GIS and a total of five chemicals (benzene, toluene, ethylbenzene, o-xylene, m,p-xylene) were modeled. Modeling results showed that among VOCs, highly volatile benzene evaporated completely within 24 h, while most of the toluene, ethylbenzene, and m,p-xylene evaporated within 48 h. Based on these results, it is suspected that people who participated in cleanup activities in the initial stage of the accident were most exposed to the VOCs.
Among 16 PAHs, naphthalene, which has the highest content and is highly volatile, mostly evaporated within 15 days, while acenaphthylene, acenaphthene, fluorene, and phenanthrene evaporated within 30 days. At the time of the accident, the amount of alkylated PAHs released was 300–400 times higher than PAHs. Although their levels were gradually decreasing since the accident, they continued to show high concentrations even 1 year after the accident. Therefore, they were suspected to have a health effect on residents who continue to participate in the cleanup activities.
19.3.4.2. Assessment of the Biomarkers
19.3.4.2.1. Exposure Biomarker
Analysis of VOC and PAH metabolites, along with heavy metals, was conducted on the urine samples collected during the health examinations of crude oil spill area residents. The geometric mean of urinary t,t-muconic acid concentrations was lower in the cleanup area (0.037 mg/g Cr) than in the affected area (0.053 mg/g Cr), but the difference was not statistically significant. The urinary 1-hydroxypyrene concentration (geometric mean) was higher in the cleanup area (0.095 μg/g Cr) than in the affected area (0.071 μg/g Cr), but the difference was not statistically significant. However, the urinary 2-naphthol concentration (geometric mean) was significantly higher in the cleanup area (2.19 μg/g Cr) than in the affected area (1.49 μg/g Cr). The blood lead concentration (geometric mean) was significantly higher in the cleanup area (3.43 μg/dL) than in the affected area (2.92 μg/dL). Residents of both the cleanup and affected areas showed higher blood lead concentration than 2.66 μg/dL—the national representative level in 2005. Furthermore, children (2.24 μg/dL) showed higher blood lead concentration than the 1.38 μg/dL reported in the fourth US National Health and Nutrition Examination Survey (NHANES), but lower than the 3.16 μg/dL reported in the fourth German Environmental Survey (GerES IV). Urinary cadmium was also significantly statistically higher in the cleanup area (1.72 μg/g Cr) than in the affected area (0.93 μg/g Cr). Residents who exceeded the 5 μg/g Cr, the value recommended by the German HBM II, were found in both the cleanup and affected areas. Urinary mercury concentrations were also statistically significantly higher in the cleanup area (0.69 μg/g Cr) than in the affected area (0.62 μg/g Cr). Because concentrations of urinary mercury can vary in people according to their dietary habits and lifestyles, even if they live in the same region, additional epidemiological studies that take into account the source of exposure and regional characteristics were planned.
19.3.4.2.2. Effect Biomarker
For identification of oxidative stress biomarker levels in oil spill area residents caused by hazardous substances, MDA, a lipid oxidative damage indicator, and 8-hydroxydeoxyguanosine (8-OHdG), a DNA oxidative damage indicator, were analyzed with the subjects divided into three groups of the cleanup area (high-exposure area), the affected area (low-exposure area), and government employees.
Urinary MDA concentrations based on the place of residence were analyzed after adjusting for gender, age, and urinary cotinine level. The results showed that the concentrations were significantly statistically higher in the cleanup area (4.57 μmol/g Cr) than in the affected area (3.11 μmol/g Cr). Urinary 8-OHdG concentrations were also analyzed after adjusting for gender, age, and urinary cotinine level. The results showed that the concentrations were significantly statistically higher in the cleanup area (5.73 μg/g Cr) than in the affected area (3.71 μg/g Cr). Analysis of urinary MDA concentrations based on the cleanup activities participation status showed that the group that participated in the cleanup activities had significantly higher urinary MDA and 8-OHdG concentrations than the group that did not participate. Moreover, an increase in the cumulative total number of days participating in the cleanup activities showed a pattern of increase in urinary MDA and 8-OHdG concentrations [14].
Analysis of oxidative stress biomarkers based on the levels of exposure to heavy metals showed that blood lead concentration was significantly correlated with urinary 8-OHdG. In addition, an increase in urinary cadmium concentrations was significantly correlated with an increase in urinary MDA concentrations. There was no significant difference in oxidative stress biomarkers based on the levels of t,t-muconic acid, which is a metabolite of benzene. As urinary 1-hydroxypyerne level increased, urinary 8-OHdG and MDA concentrations also showed a significant increase.
19.3.4.3. Health Effects in Adults
Health surveys on adults included questionnaires, general health examinations, pulmonary function tests, and chest radiographs. Three types of exposure variables were constructed for analysis: the distance from the contaminated coast to residence after the initial accident, duration of cleanup activities, and level of exposure biomarkers. Relationships between each of the different exposure variables and health effects were analyzed. Being closer to the contaminated coast after the initial accident was associated with a longer duration of cleanup activities, and an increase in estimated individual exposure level was seen accordingly.
The questionnaire survey on subjective physical symptoms demonstrated that such symptoms were associated with the duration of cleanup activities and how much oil had come into contact with the skin. As the duration of participating in the cleanup activities increased, the rate of eye irritation, nasal irritation, headache, fatigue/fever, musculoskeletal symptoms, memory/cognitive disturbance, and back pain also increased significantly. The symptom rate of nasal irritation, sore throat, and memory/cognitive disturbance appeared significantly higher in cases where the amount of oil coming in contact with the skin was “very much” [6].
With respect to allergies, a longer, total cleanup activity period showed to significantly increase the rate of allergy symptoms and the onset of allergy symptoms in the past year from the oil spill to the survey. A significant increase in the diagnosis rate of dermatitis or conjunctivitis associated with an increase of total cleanup activity period.
Multiple chemical hypersensitivity syndrome showed statistically significant dose–response relationships with cleanup activity and distance indicators, just as the allergy symptoms questionnaire survey did.
The total cleanup activity period from the accident to the survey, cleanup period from the accident until 1 month later, and distance from the contaminated coast at the early stage of the accident to residence showed associations to various health outcomes. In contrast, exposure biomarkers and health effects did not show significant associations.
19.3.4.4. Health Effects in Children
The health surveys related to children included questionnaire surveys, general health examination, pulmonary function tests, skin prick tests, and methacholine provocation tests. The questionnaire survey showed that the positive response rate in asthma symptoms, diagnosis, and treatment was high in subjects from coastal regions or regions close to the oil spill area. The pulmonary function test, predicted forced vital capacity (FVC), and forced expiratory volume in 1 s (FEV1) values were lower in the high-exposure group. The methacholine provocation test results showed significantly higher prevalence in the subjects from the high-exposure area [15].
The results suggest that children who live near the oil accident site face a greater possibility of being exposed to hazardous substances by various routes that can affect asthma.
19.3.4.5. Mental Health and Psychosocial Care Programs
The Taean oil spill was an accident which occurred close to where the residents live and to residents whose livelihood relied mostly on fishing and aquafarming, and the accident not only brought about economic damage, but also destruction of their livelihood. Such accidents can cause psychological stress and have a major effect on mental health, causing depression or suicidal ideation. An acute health survey following the accident showed that the levels of psychosocial stress, depression, and suicidal ideation in Taean residents were 1.2–4 times higher than the general population. These results showed significant associations with the distance from the residence being closer to the accident site and working in fisheries or tourism.
These results suggested the need for an in-depth investigation of the psychosocial state of Taean residents and programs designed to promote their health. Therefore, mental health assessments and health promotion programs were conducted on the residents. Mental health assessments involved measurements of PTSD, depression, and anxiety, which were measured using the PDS, CES-D, and STAI, respectively. PTSD, depression, psychosocial stress, trait and state anxiety were all significantly higher in the cleanup area (high-exposure area). A total of 23–40% of the residents were identified as being in the high-risk group for PTSD and depression—raising long-term health concerns.
Health promotion programs for the residents and children included consultations, educational projects, and mental health camps. A post hoc assessment was conducted on mental health after these programs were implemented.
In the programs for children, screenings for state anxiety, ADHD, depression, and PTSD in primary school students included even diagnoses by tertiary health professionals, and along with the tests, parent education was also provided. This gave parents awareness of the overall mental health issues faced by their children. Personal mental health consultations and group consultations were conducted for children who required mental health consultations, which brought about a reduction in PTSD and state anxiety, as well as an improvement in their mental health.
To promote the residents' awareness of the mental health issues associated with the adverse effects of the oil spill exposure, mental health meetings for local residents were held to foster their ability to manage mental health problems and stress on their own. In addition, laughter therapy and anger management program were conducted, and through the program, we found that both state anger and trait anger were reduced after the program and anger was well-managed. Assessments revealed that mental health status improved in all categories after the programs.
19.3.5. Second Long-Term Health Survey
The second medium- to long-term health survey on adults was conducted between October and November of 2010, 3 years later since the accident, and included 1257 residents from the high-exposure area. The survey on children was conducted between March and April of 2011 and included 760 participants. The survey consisted of a questionnaire, health examinations, and specialized tests [16].
19.3.5.1. Health Survey in Adults
19.3.5.1.1. Oxidative Stress Biomarkers
Oxidative stress biomarkers were analyzed in 270 people whose MDA and 8-OHdG were analyzed during both the first and second health surveys. Among 270 subjects, 240 subjects (88.9%) participated in the cleanup activities during December 2007 when the accident occurred, while 30 subjects (11.1%) did not participate. Therefore, most of the subjects participated in the cleanup activities during the acute stage. Concentrations of 8-OHdG and MDA showed no difference between the participant and nonparticipant groups in the cleanup activities during the acute stage when adjusted for gender, age, and urinary cotinine concentrations.
Urinary oxidative stress biomarkers levels based on the number of days of participation in the cleanup activities in December 2007 were analyzed, adjusted for gender, age, and urinary cotinine concentrations. The results also showed no differences in 8-OHdG and MDA between the groups which did not participate, participated for <14 days, and participated for ≥14 days.
With respect to urinary oxidative stress biomarkers levels based on the distance from residence to contaminated coast at initial stage of the accident, a 2009 study showed higher urinary 8-OHdG concentrations in those with shorter distance. However, urinary 8-OHdG concentrations did not show significant differences in 2010. Urinary MDA also did not show significant differences with the distance from residences to the contaminated coast at the initial stage of the accident in the 2009 survey, and did not show significant differences with MDA concentrations in 2010 as well. However, urinary MDA level in 2010 was correlated with levels of urinary cadmium in 2009, 2010, and urinary mercury in 2010.
Urinary 8-OHdG concentrations of high-exposure area residents showed very little reduction from 2009 to 2010 with values of 5.87 μg/g/Cr and 5.61 μg/g Cr, respectively. Furthermore, those values were higher than the geometric mean value of 4.39 μg/g/Cr found in the group of low-exposure area residents who participated in the cleanup activities in 2009. Therefore, the results demonstrated that no significant recovery had taken place over time and suggested the potential for delayed health effects on the residents. Meanwhile, urinary MDA concentrations showed a statistically significant decrease from 2009 to 2010, with values of 3.48 and 2.40 μmol/g Cr, respectively.
19.3.5.1.2. Respiratory Health
Out of roughly 10,000 subjects of the first health survey, 527 residents who showed abnormal findings in the pulmonary function test and X-ray exam were chosen to form a panel. A questionnaire survey, bronchial sensitivity test, bronchodilation test, and skin prick test were performed on the panel. Excluding those with health problems and those who voluntarily refused to participate, a total of 417 people underwent bronchial sensitivity tests (n = 322) and bronchodilation tests (n = 95). For the skin prick test, other than the positive control (saline) and negative control (histamine), tests were performed on a total of 12 antigens: house dust mites (American-type: Dermatophagoides farinae; European-type: Dermatophagoides pteronyssinus), cockroach, grasses, Tree-1, Tree-2, mugwort, Hop japanese, ragweed, cat fur, Mold-1, and Mold-2.
Of the 322 people who were given a bronchial sensitivity test (methacholine provocation test), 99 people (30.8%) tested positive. Among the subjects, a total of 95 people who were unable to receive a bronchial sensitivity test due to having a FEV1 ≤70% were given a bronchodilation test: of which, 45 people (47.4%) tested positive.
Among 527 subjects who received a skin prick test, 49 people (9.3%) tested positive for at least one of the 12 antigens.
A panel survey of 526 adults who complained of asthma symptoms, however, showed no significant association between the number of days participated in the cleanup activities and a definitive diagnosis of asthma.
Comparisons of changes in pulmonary function over time showed that FVC (%) significantly decreased in 2010 compared to that in 2009. Pulmonary function tests based on participation in the cleanup activities showed that the group, which participated in the cleanup activities had significantly reduced FVC (%), but there was no difference in FEV1/FVC.
19.3.5.2. Health Survey in Children
19.3.5.2.1. Oxidative Stress Biomarkers
In 290 children out of 495 children who participated in the first health survey, oxidative stress biomarkers were analyzed by participating in the follow-up second survey. Among the subjects, 156 children (53.8%) visited the accident site after the oil spill, while 71 (24.5%) participated in the cleanup activities. Most of the children participated in the cleanup activities for less than a day. There were no differences in oxidative stress biomarker concentrations based on the distance between the accident site and residence or school. Participating in cleanup activities for longer periods of time resulted in increased urinary 8-OHdG and urinary MDA concentrations, but the differences were not statistically significant.
With respect to the recovery of oxidative stress biomarkers over time, girls showed slower recovery in oxidative stress biomarker levels than boys. The MDA levels in girls actually increased by 1.5 times as compared to the first survey while the 8-OHdG levels decreased significantly.
19.3.5.2.2. Respiratory Health
Among the 1172 children who participated in the first health survey, 760 children who were followed-up with were analyzed using a questionnaire, skin prick test, pulmonary function test, and bronchial sensitivity test.
With respect to the respiratory health effects in children, despite the fact that 3 years had passed since the accident, the asthma symptom rate was still significantly higher in those who resided or attended school a shorter distance from the accident site. In the skin prick test, distance from residence to the accident site and from school to the accident site did not show significant associations. With respect to pulmonary function, significantly better values were seen in secondary school students than those in primary school, and in boys than girls.
Meanwhile, FVC and FEV1 were significantly lower in the group who lived <20 km from the accident site than in the group who lived ≥20 km away, particularly in primary school students. The pulmonary function of the high-exposure group showed significantly lower values than the low-exposure group with respect to FVC (% pred) and FEV1 (% pred). An additional bronchial sensitivity test was performed on 70 people who reported symptoms of asthma from the standardized questionnaire to make a definitive diagnosis of asthma. As a result, increased diagnoses of definitive asthma based on the distance from school or residence to the accident site were seen, but the differences were not statistically significant.
Based on these results, it was determined that despite the fact that 3 years had passed since the accident, its effects on the respiratory health of children and adolescents residing in the oil spill damaged area still remained, and such effects were greater in primary school students (children) than in secondary school students (adolescents). It is believed that this is due to younger children being relatively more vulnerable to contaminants.
19.3.5.3. Burden of Disease
The burden of disease (BOD) in the damaged area from the oil spill was quantified based on 10,171 people who participated in the first health survey. BOD calculation takes into account the distribution of the exposed population and quantifies the health effects on the damage area residents. It can be used as an evidence for future damage cost calculations and the establishment of and support for recovery plans. To quantify the BOD, the present study used the disability-adjusted life years (DALY) developed and used by the World Health Organization (WHO).
For calculation of attributable BOD, the temporal range used 2008 as the reference. In the BOD calculation, the excess occurrence of oil spill–related diseases was estimated through comparison with prevalence found in control regions with no contamination.
Disability weights, including physical and mental diseases, were calculated based on 10,171 people from the 2008 survey. Years lost due to disability associated with the oil spill was estimated from 14,724 DALYs from the 2008 survey. The results were similar between the genders with 7425 DALYs for males and 7299 DALYs for females. However, there were differences for individual diseases. Males showed a high BOD for mental diseases, such as PTSD and depression, while females showed a higher BOD for allergies, including conjunctivitis, dermatitis, and rhinitis, as well as asthma [17].
The BOD of asthma among the damaged area residents was 6138 person-years, which accounted for approximately 36% of all the BOD of the residents: making it the highest BOD among all diseases being studied. Moreover, the sum of BODs for asthma, allergies, and multiple chemical sensitivity was the highest among those in their 40s and 50s, while mental disorder had the highest BOD among those in their 20s. Overall, the highest BOD was found among those in the 40s, which was due to the fact that the population in the damaged area had higher percentages of people in their 40s and 50s.
The study had the limitation of not reflecting the BOD for chronic diseases, such as hypertension, hyperglycemia, cardiovascular diseases, and metabolic disorders. Because data related to diseases that increased before and after the accident were not obtained, they could not be included. The oxidative stress biomarkers 8-OHdG and MDA are known to be associated with various cancers and chronic diseases. Considering that the oxidative stress biomarker concentrations were significantly higher in the high-exposure area, it is necessary to continue BOD studies on damaged areas that reflect the medium-to long-term health effect results on additional cancers or chronic diseases.
19.3.6. Key Findings of Health Effects After Second Health Survey
19.3.6.1. Adult Oxidative Stress Biomarkers
The survey conducted one and a half year after the accident (the first and second surveys) showed that both oxidative stress biomarkers 8-OHdG and MDA were significantly higher in the high-exposure area residents who lived closer to the accident site than in low-exposure area residents. In addition, both 8-OHdG and MDA showed higher concentrations in those who participated in the cleanup activities for fewer days and those who participated in the cleanup activities for more days.
The survey conducted 3 years after the accident (the third survey) studied only the high-exposure area residents and showed that cleanup activities participation status and duration were not significantly correlated with oxidative stress biomarkers' level. The high-exposure area residents showed a significant decrease in MDA concentrations 3 years after the accident, as compared to one and a half years after the accident, but showed very little difference in 8-OHdG concentrations.
The follow-up survey conducted 6 years after the accident (the fourth survey) aimed to identify the levels of oxidative stress biomarkers and level of recovery over time in both the high- and low-exposure area residents. Of the 802 people who participated in the fourth survey, a total of 304 cases were analyzed. A total of 173 cases from the high-exposure area and 131 cases from the low-exposure area were analyzed for oxidative stress biomarkers starting from the first survey.
Urinary MDA and 8-OHdG concentrations in study subject from damaged area 6 years after the accident, after adjusting for confounding, were higher in the high-exposure group than in the low-exposure group. Oxidative stress biomarker levels based on the area classification and number of days participating in the cleanup activities also showed the highest oxidative concentrations in the group consisting of high-exposure area residents who participated in the cleanup activities for a long time with a dose–response relationship.
Changes in oxidative stress biomarker levels over time conducted one and a half and 6 years after the accident were examined in the high and low exposure groups. Urinary MDA concentrations significantly decreased after 6 years but 8-OHdG concentrations did not. Existing studies have reported that these oxidative stress biomarkers affect chronic diseases such as metabolic disorder and cancer, therefore, studies linked to chronic diseases are needed in the future.
19.3.6.2. Respiratory Health Effects in Children
To examine whether the oil spill continued to affect the respiratory health of children even 5 years after the accident, the third health survey on 783 children and adolescents in the damaged area was conducted in 2013. The respiratory health examination including a questionnaire survey, skin prick test, pulmonary function test, and exhaled nitric oxide test (lung, bronchial inflammation) was performed on 531 primary school students. The primary schools being surveyed were divided into five high-exposure area schools, which are located in towns close to the coasts contaminated by a thick layer of oil during the initial stage of the accident, and seven low exposure area schools, which are inland and relatively further away from the coast.
Questions from a standardized questionnaire for measuring allergies, the International Study of Asthma and Allergies in Children (ISAAC), were used to measure the complaint rate for asthma symptoms. The results showed that among 531 children in the damaged area, prevalence of “experiencing lifetime asthma symptoms” was 13.7% (n = 73) and “asthma diagnosis” was 12.6% (n = 67). Among the 67 children who were diagnosed with asthma, 30 children responded that they were diagnosed with asthma after the oil accident. The diagnosis rate for asthma was higher in boys than in girls.
Among the total of 531 study subjects, the number of those who visited the accident site within 1 year of the accident was 234 (44.1%) and those who visited in December 2007, within 1 month of the accident was 139 (26.2%). Very few children, 17 (3.2%), participated in the cleanup activities. The experience of visiting the accident site within 1 year of the accident had a significant influence on asthma symptoms and asthma diagnosis in the children from the damaged area. The prevalence of “asthma symptoms” and “asthma diagnosis” was significantly higher in children who visited the accident site than in those who did not.
Despite the fact that 5–6 years have passed since the accident, the prevalence of “asthma symptoms” and “asthma diagnosis” in these children remain higher than the national average for children. In the skin prick test, 160 out of 531 children (30.3%) tested positive for at least 1 of the 12 antigens. The positivity rate in children who visited the accident site was higher than that of children who did not visit the accident site, but the difference was not significant. From the FVC and FEV1 results of the pulmonary function test, whether children visited the accident site within 1 year of the accident had a significant influence on their pulmonary function was examined. The FEV1/FVC (%) was significantly lower in children who visited the accident site within 1 month of the accident compared to children who did not.
In conclusion, the analysis of respiratory health effects on children 5–6 years after the accident (the third survey), with the distance from school to the accident site as the exposure variable, showed that no significant differences were found between the high and low exposure groups with respect to “asthma symptoms,” “asthma diagnosis,” skin prick test results, and pulmonary function test results. On the other hand, whether a child had visited the accident site or not was a variable that showed significant differences in “asthma symptoms,” “asthma diagnosis,” and pulmonary function. These findings confirmed that even though 5–6 years had passed since the accident, the oil spill continued to have a negative effect on the respiratory health of children in the damaged area. It is necessary to strengthen asthma management and health promotion programs that can enhance the health levels of children in the damaged area.
19.4. Mothers and Children's Environmental Health Study
In order to monitor health effects on mothers and infants after the Hebei Spirit oil spill, as a part of the mothers and children's environmental health (MOCEH) study which was a multicenter prospective birth cohort study initiated from 2006, 80 pregnant women in Taean area were recruited since 2008 and follow-up monitoring was conducted on the newborns.
The MOCEH study included a questionnaire survey, biological sample test, Bayley Scales, infant intelligence test, fetal growth and development test, allergy test, and dietary intake survey. The questionnaire survey was conducted on mothers who gave their consent for participation and the mothers filled out the questionnaire at 6, 12, 24, 36, 48, and 60 months after giving birth. Both the mother and the spouse received the questionnaire that surveyed general characteristics, breastfeeding, health status of the parents, disease history of the parents, nursing environment, socioeconomic status, housing environment, living environment, and dietary intake. Biological sample tests included testing of urinary PAH and VOC metabolites, endocrine disruptors (bisphenol A, phthalate), and blood heavy metal concentrations. To measure the infant growth and development, anthropometric measurements, neurocognitive development tests, children's intelligence development tests, and allergy tests were performed. The Bayley Scales of Infant Development was used for a neurocognitive development test and Korean-Wechsler Intelligence Scale for Children (K-WISC) was used for an intelligence development test.
Questionnaires, Bayley Scales, and dietary nutrition surveys were performed as a follow-up survey on the infants. Of the 77 mothers or infants, who participated in any of the health surveys from the early stage of pregnancy to when the child was 60 months old, 18 (23.4%) were from the high-exposure area and 59 (76.6%) were from the low-exposure area. The MOCEH study showed that children in the high-exposure group had significantly higher prevalence of atopic dermatitis and other allergic diseases (allergic rhinitis, allergic conjunctivitis, and food allergies) than those in the low-exposure group. Since mothers and children both represent groups that are sensitive to hazardous substances, continued studies are needed. Accordingly, the TEHC participated in the Korean Children's Environmental Health Study, an ambitious prospective project aimed to recruit 100,000 pregnant women initiated by the MOE, in an effort to conduct studies for identification of health effects from environmental exposure.
19.5. Environmental Health Contingency Plan in Oil Spill Disasters
Marine oil spill accidents can occur from various causes, including crashes, bad weather, stranding, and sinking. Because South Korea has a high dependency on crude oil as a source of energy, and consequently, it is a country in which oil spill accidents occur often due to frequent traffic of large oil tankers. In the case of Taean oil spill, because of the lack of a systematic and timely government health response to the accident in its initial stage, residents in areas contaminated by the accident in its initial stage were exposed to high levels of environmental contaminants, such as PAHs, VOCs, and heavy metals. Because there was no systematic monitoring of hazardous substances, such as VOCs, released into the atmosphere in the initial stage of the accident, scientific and systematic work on the assessment and monitoring of environmental and health effects was not performed. Therefore, when disasters such as oil spills occur, an appropriate rapid response is critical to minimize the damage.
According to an MOE study conducted after the Hebei Spirit oil spill, the WHO developed environmental health measures to respond to environmental health emergencies and disasters, but cases of response according to the manuals in actual disasters are rare [1]. The reason is because it is difficult to apply a generalized response strategy to disasters which have different types of occurrence and damage. Therefore, it is necessary to establish a detailed response strategy for each individual disaster.
When disasters, such as oil spills, occur, there are four basic principles for minimizing national health effects. First, establish thorough prevention and safety management measures to prevent accidents. Second, identify and give preferential considerations to the vulnerable population. Third, give preferential considerations to the susceptible group, including pregnant women, children, and the elderly living alone. Fourth, establish a long-term response system and recovery plans for complete recovery of health and community [18].
Under these principles, the establishment of environmental health action guidelines following the oil spill accident can be divided into two stages; preparation and response [19]. In the preparation stage, necessary tasks include: (1) communication on risks before accidents; (2) identification of types and properties of hazardous substances and construction of possible scenarios; (3) promotion of environmental health action guidelines during accidents (items needed for reducing damage and action guidelines for exposure to oil); (4) identification of the vulnerable population and susceptible groups and establishment of evacuation plans; and (5) prior training and education.
In the response stage, necessary tasks include: (1) establishment of emergency action guidelines (establishment of cleanup instructions); (2) establishment of evacuation plans for susceptible groups and hygienic care during evacuation; (3) implementation of environmental monitoring (acute exposure assessment list and assessment techniques); and (4) conduct health surveys (prioritization and selection of items for health effect assessment). Especially in the case of susceptible groups that require special measures, such as infants and pregnant women, action guidelines for them must be prepared very quickly. Such action guidelines and evacuation plans need to be prepared with identification of the population under potential risk based on the amount of oil spilled, types of hazardous substances, where the oil spill occurred, and how it is being dispersed.
In order to implement such a response system, it is necessary to have institutional measures that can support the system in place. First, active cooperation from and preparation by the MOE, Ministry of Health and Welfare, and Ministry of Labor is needed. Moreover, it is necessary to form an “Environmental Health Support Group” comprising environmental health experts and personnel from relevant departments. This group will be in-charge of undertaking the tasks involved in the identification of and preparation planning for at-risk population, vulnerable groups, and susceptible groups based on each oil dispersion scenario; establishment of hygienic plans during evacuation; conduct environmental exposure assessment; establishment of health protection plans for workers and residents during coastal cleanup activities; prioritization and selection of items for health survey; and preparation of emergency response measures against risk factors for environmental health.
Second, it is necessary for MOE to strengthen the role and responsibilities from relevant agencies to the lead agency when an environmental disaster occurs.
Third, for efficient environmental health countermeasures, environmental health–related agencies must have leaders and trained personnel with experience in responding to oil spills in place, as well as proper transport and logistics support systems, regulations, and guidelines. In order to achieve this, an environmental health manager or leader must be designated at the national or local government level, and postaccident response training must be conducted at all times and include relevant agencies.
Fourth, on-site broadcasts must include information on the hazards of crude oil, action advices, action guidelines for susceptible groups, and emergency measures promotion plans.
Fifth, long- and short-term health recovery plans and support plans for community restoration must be prepared [20].
19.6. Future Needs
The health effects from the Taean oil spill showed a trend of recovery over time but some parts were still affected or the health effects remained. Oxidative stress biomarkers, such as 8-OHdG, still showed a significant correlation with level of exposure, even 6 years after the accident. Based on these results, the directions needed for a long-term health study on Taean oil spill are as follows:
First, there is a need to identify the biological mechanisms and causal relationships of associations between adverse health and the oil spill exposure through toxicological studies. DNA oxidative stress biomarkers still appearing at high levels in the exposed area indicates that the residents in this area may be vulnerable to chronic diseases related to this indicator, such as cancer, diabetes, degenerative diseases, and endocrine disorders. Reports on cytogenetic and toxicological studies related to oil spills include meaningful results from studies on the Prestige oil spill of Spain [21–23]. From an epidemiological perspective, it is difficult to accurately establish a causal association; toxicological, genetic, and epigenetic studies including animal experiments are needed.
Second, follow-up surveys of volunteers and military personnel who participated in the cleanup activities during the initial stage of the accident are needed. Of the 122,296 people who participated in the cleanup activities following the accident, approximately 560,000 were residents and 1,230,000 were volunteers. The number of volunteers peaked at 38,875 on December 27, 2007 and gradually decreased thereafter. In the initial stage of the accident, the cleanup activities at the accident site and contaminated areas were performed by military personnel and coast guards as the work required a level of expertise. It is suspected that they were exposed to significant levels of initial VOCs and PAHs. Initial acute health survey results showed that the concentrations of some heavy metals and VOC and PAH metabolites were higher in these volunteers, as compared to the general public, which confirmed that these levels of exposure had a significant effect on health. Therefore, the coast guards and military personnel who were working on the frontline during the accident had a high probability of having health effects similar to the residents of the contaminated area. Consequently, it is needed to compare this large group of volunteers who participated in the cleanup activities with a population that was not exposed to the oil spill to determine whether they had higher disease incidence rates. If direct investigation is deemed difficult, then the level of exposure can be identified and national statistical data can be used to assess the effect of oil spills on occurrence of diseases.
Third, research linked to ecological studies is needed. The livelihood of Taean region is dependent on the ocean and tidal flats, and the residents consume seafood and crops harvested from the region. Restoration of the ecosystem is an important variable in secondary health effects, as well as an important item for assessment of chronic health effects. Therefore, future studies on health risk levels in association with ecotoxicology and level of ecological restoration will be important for more in-depth assessment of health effects on the residents.
Fourth, activation of health promotion projects for the residents, based on the health survey results to date, is needed. Risk communication for the residents should become commonplace, and customized programs for promoting health status diminished by the oil spill should be planned and pursued. In particular, psychosocial projects for improving mental health of the residents are important. Screening high-risk groups who are suffering mental health issues caused by the oil spill among the residents and continuing to implement treatments and consultations for them are needed.
Fifth, international collaboration on oil contamination–related health studies is needed. Currently, oil contamination accidents in specific areas occur rarely, which makes it difficult to develop experts. This creates a situation that does not allow appropriate preaccident planning and postaccident response has to be implemented. Particularly in the field of health effects, studies and data are lacking, thus, findings from each study should be shared to compile diverse and in-depth findings on oil spills and its health effects. Research topics, methodologies, results, and trends should also be shared, and if possible, collaborative studies can be conducted to publish findings on oil spills and health effects, with which to establish environmental health policies. In order to accomplish this, it is necessary to establish a network between existing researchers as a system of sharing the cumulative knowledge and experience from each country, in addition to engaging in active exchanges.
Acknowledgments
The health projects on Hebei Spirit oil spill conducted by the Taean Environmental Health Center (TEHC) was financially supported by the Ministry of Environment, local governments of Chungcheongnam-do and Taean-gun since 2008.
We appreciate Drs. Jongil Hur, Wool-Chul Jeong, Ik-Jin Lee, and Mr. Yong-Jin Jeon and Ms. Eun-Young Cho for their enthusiastic dedications to establish the baseline cohort of the health survey at the founding periods of the TEHC. We are thankful to Ms. Su Ryeon Noh, Eun Kyung Yang, Jung Ah Kim, Yeonhee Chu and Mr. Gwi Heum Eom for the successful accomplishment of the followed health surveys and collecting the data. We particularly appreciate Dr. Yong Hyun Choi, the director of Taean Environmental Health Center, for his passionate support to all works. We are also thankful to many citizen's environmental organizations and experts who are devoted to investigation of acute health effects of oil spill.
..................Content has been hidden....................
You can't read the all page of ebook, please click here login for view all page.