
7. The Top Healthcare Analytics Adaptations
There is a common thread running through the analytics adaptations. Simply said, the way to improve outcomes is to ramp up the involvement of people in the co-production of their health.
This chapter presents a distillation of the ideas generated throughout the book into seven healthcare analytics adaptations. These adaptations emerged from the adaptations discovery process described in the first chapter. The ideas chosen for development into adaptations are the truest representation of the industries’ sweet spots and the most amenable to shaping into solutions. They also happen to address significant challenges in health and healthcare.
Seven Adaptations
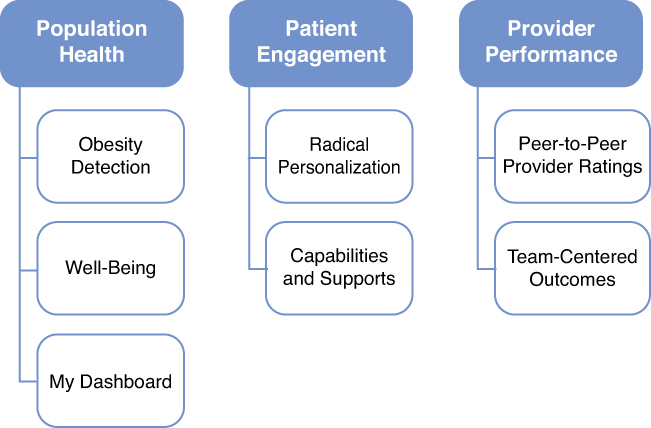
The seven analytics adaptations cluster into three important areas of health and healthcare, including population health, patient engagement, and provider accountability. Figure 7.1 shows how each of the adaptations maps to the clusters. The adaptations for Population Health include obesity detection, well-being, and my dashboard. For Patient Engagement, the adaptations include radical personalization and capabilities and support. Provider Performance includes the adaptations of peer-to-peer provider performance ratings and team-centered outcomes.
Each adaptation is described in terms of the business need and business goal, the industry derivation including the relevant analytic sweet spots, the analytics goal and associated methods, and the major challenges for adopting the analytics into practice. Note that the next chapter presents a how-to framework for evaluating and progressing an adaptation through the adoption decision stage of the Innovation Pathway, a framework for the journey of an innovation from the idea stage to its successful implementation and reinvention. A hypothetical case study addresses the many issues at play for successful adoption and uses the Innovation Adoption Factors Model as a guide.
Obesity Detection
The first analytics adaptation addresses the challenge of reducing the burden of chronic diseases through early identification and intervention (see Table 7.1).
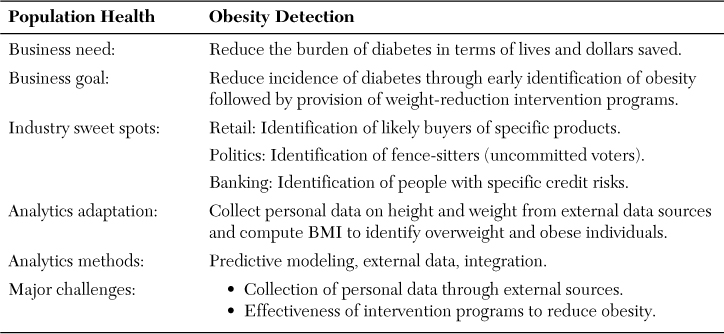
This adaptation specifically focuses on the business need to reduce the burden of diabetes in terms of lives and dollars at stake. It homes in on obesity, a very serious epidemic and a major precursor of diabetes. The business goal is to reduce the incidence of diabetes through early identification of an individual’s premorbid obesity, which is followed by targeted intervention programs to reverse weight gain. Many of these individuals will not have received sickness care, or might have received it for other reasons that did not include a risk assessment for diabetes. Therefore, there might not be any relevant data included in a traditional medical record that speaks to obesity. The analytics of multiple industries converge on this adaptation. Retail, banking, and politics have multiple data sources and sophisticated analytics to identify likely buyers, uncommitted voters, or probable defaulters, and they have programs to sell, convince, or reject those so identified.
The analytics adaptation is straightforward. The determination of the degree of obesity is easily determined by a simple calculation of the two variables of height and weight. The data are available from firms that aggregate publicly available data (and are not easily available from claims or medical records). The analytics methods include predictive modeling and the collection and integration of external data. The major challenges are belief systems that question the utility and appropriateness of external data and whether interventions intended to reverse obesity are effective.
Well-Being
The second analytics adaptation addresses the challenge to measure the health of populations in the way it is defined by the World Health Organization, that is, well-being (see Table 7.2).

The measurement of well-being can have implications about the structure and intent of delivery systems because what is measured tends to get managed. This will facilitate stretching the historical boundaries of sick care to include total health. In addition to influencing the definition of what constitutes success, this adaptation has a direct purpose to measure what is important to people and thereby to earn their interest and engagement.
The business need is to activate people to co-produce health. The business goal is to reframe what success looks like from the customer’s perspective to improve trust, exchange of information, and outcomes. The industry sweet spot comes from politics. Polling during presidential elections has been very effective in eliciting lots of pertinent data from voters.
The analytics adaptation is to use polling, or surveying, to determine well-being for a health plan, delivery system of municipality using an established, credible, and cost-effective approach. The suggestion is to use the Behavioral Risk Factor Surveillance System (BRFSS) on selected measures, oversampling for the specific population of interest. The data collection and analysis is mostly outsourced to the CDC. The analytics methods for a health plan or delivery system are mostly in the reporting, through customer-centric dashboards and the coupling of the information with other analytics adaptations, including social media.
The challenges include beliefs that there might be mission creep if healthcare expanded its purpose to address well-being. Also, there might be an unfamiliarity and discomfort with using publicly available databases.
My Dashboard
The third analytics adaptation also addresses the business need to activate people to be contributing partners in co-producing their own health (see Table 7.3).
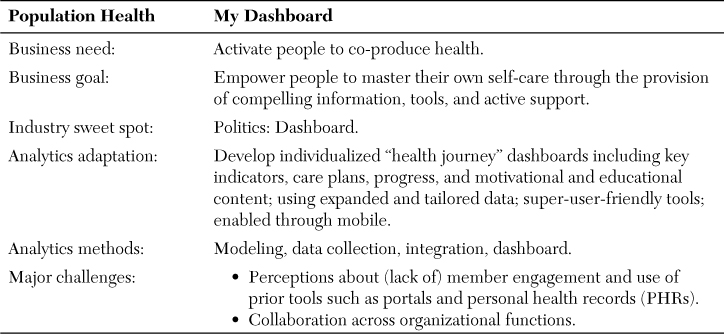
The business goal is to excite and empower people to master their own self-care through the provision of compelling tools and active support. This addresses a blind spot related to the paradox that clinicians need well-designed clinical support systems to provide optimal care, but patients do not and are essentially relegated to the role of recipients, but not participants, in using information to make important decisions about their care. The industry sweet spot, again, is politics. The dashboard developed and used by the winning presidential candidate in 2012 was lauded as a major factor in empowering campaign workers to persuade voters and get them to vote. This, in combination with other data-driven approaches, was the major factor in winning the election.
The analytics adaptation is an individualized “health journey” dashboard including key indicators, care plans, progress over time, decision frameworks, and motivational and educational content. It would use expanded and tailored data, use super-user-friendly tools, and be delivered through customer-preferred channels, like mobile.
The major challenges are the beliefs that member engagement through information products has been tried and failed before, including patient portals and personal health records. The existing design of these tools might not be up to the challenge. For example, some health-plan member portals are focused on getting members to fill out administrative forms more efficiently. This is not an optimal way to engage them, it underutilizes the technology, and it misses an opportunity to gain member trust. Another challenge is that the design features of such an expanded approach to a patient-centric dashboard involves a good deal of coordination and data integration across the enterprise and requires innovative new approaches to providing compelling presentations to consumers.
Radical Personalization
The fourth analytics adaptation also focuses on the business need to activate people to co-produce their own health (see Table 7.4).

The business goal focuses on capturing customer mindshare and motivating behavior change through radical customization. The industry sweet spot is from retail and it’s well developed. The model from retail is the integration of market segmentation, messaging, omni-channel communications, and focused interventions.
The analytics adaptation is to refine microsegmentation to the (nearly) individual level and leverage the needs and predilections of each cluster with targeted interventions, matched with customized messaging and channel preferences, to achieve better compliance for distinct clinical needs. An area that is particularly ripe for this approach is patient compliance/adherence with treatment orders and medication prescriptions. The primary analytics method is deep microsegmentation based on significantly expanded and diverse data obtained from external sources. Predictive modeling is needed to determine the microsegment and its impact on the dependent variable, including its interaction with messaging, channel, and intervention.
The major challenges are the “usual suspects” in this area of activating people, including the use of external data and the belief that people cannot be activated to improve their own outcomes. Also, although the approach has been well-honed by marketing customer analytics to sell products, it may be a counterintuitive leap to use it to improve health.
Capabilities and Supports
The fifth analytics adaptation addresses the challenge to improve patient engagement by supporting and activating patients (see Table 7.5).
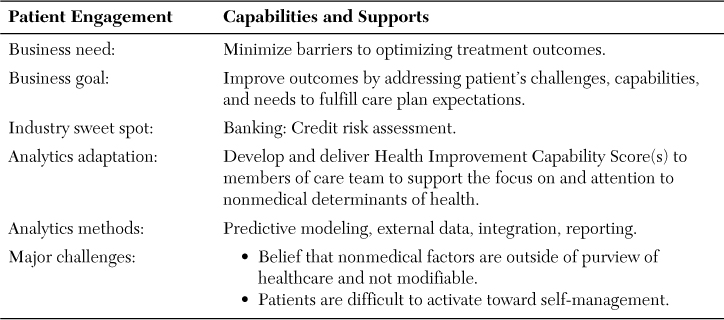
The overall business need is to improve outcomes by overcoming nonmedical barriers to successful care. The business goal is to improve outcomes by addressing the patient’s challenges, capabilities, and needs to fulfill care-plan expectations.
The healthare analytics adaptation is derived from the banking and credit industries, which have refined the measurement of risk through the use of a broad array of data and sophisticated predictive modeling. The analytics adaptation is the Health Improvement Capability Score (HICS). It is a composite score of the overall capability of a patient to succeed with treatment based on the individual’s level of activation, self-care skills, and the social determinants affecting the individual. The components of the overall score are also calculated. The scores would be made available to clinicians in the patient’s medical record and to others who coordinate linkages with nonmedical services. The HICS scores might be as important as laboratory values in setting a course of successful treatment. The analytics methods include predictive modeling to determine the key factors related to poor outcomes, the collection of new data to populate the models, data integration, and clinical decision support reporting. The analytics capability to deliver is mature in general but variable by organization. The major analytical challenges include the capacity to build the new models and develop processes to collect new data from outside the industry.
The major challenges in the adoption of the overall innovation (which the analytics adaptation supports) is the perception that nonmedical factors are outside the purview of healthcare, that they are not modifiable, and that patients are generally disengaged from their own self-care.
Peer-to-Peer Provider Performance Ratings
The sixth analytics adaptation addresses the business need to improve provider performance through measurement and transparency, but with a twist (see Table 7.6).
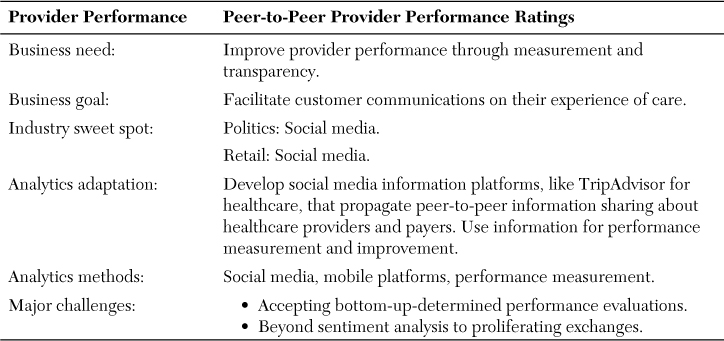
The business goal is to facilitate the expansion of customer communications about their care experiences. The rationale is that people have not been invited in or involved in providing feedback about their care to any appreciable degree, and that the information produced by experts through the traditional performance measurement approach is uninterpretable and unhelpful to people. They do not use it to make decisions about their insurers or their care, and the attempts to support this goal have been insufficient.
The industry sweet spot, from both retail and politics, is the use of social media, but not in a surveillance way to monitor sentiment. People have changed the power dynamics in other industries through mobile and social media by getting the information they need, when they want it, from trusted peers, and less so from sellers (except for price information, which they can instantaneously shop around).
The analytics adaptation is to develop social media information platforms, like TripAdvisor for healthcare, that propagate peer-to-peer information sharing about healthcare providers and payers. Healthcare can harvest this information but it cannot and should not control it, given the strong preferences exhibited by customers in other industries to eschew information domination from sellers.
The analytics methods include an understanding of social media and mobile and how to facilitate their use among the crowd of customers. The major challenges include existing beliefs about the nature of performance measurement, uncertainty about the benefits of social media, and relying on customers to lead the way on using information networks.
Team-Centered Outcomes
The seventh analytics adaptation addresses the business need to improve provider performance (see Table 7.7).
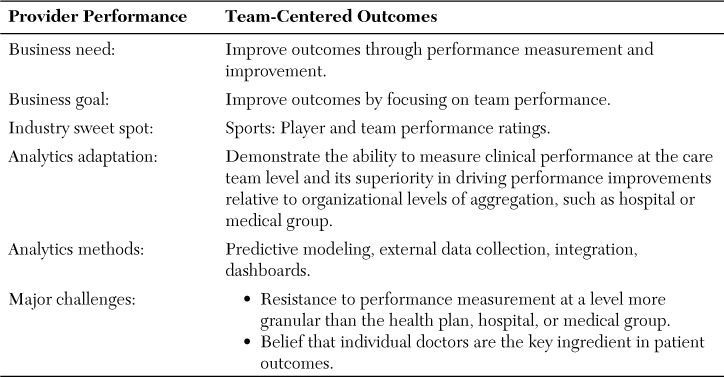
The business goal is to improve outcomes by focusing on team performance. The industry sweet spot comes from sports, where performance measurement of individual players, along with full transparency, has been a mainstay of the industry.
One could focus on the paradox that consumers know much more about their sports heroes than about their doctors though they should know more about a doctor’s “batting average.” But we take a different view. Performance measurement of players has been more about entertainment than about winning games. The pressures on the business of sports have moved the measurement to outcomes (winning) and how the combination of player attributes and individual performance contribute to team wins. Indeed, the sports industry now realizes that after decades of concentrating on individual performance, the business needs to make teams work better.
The analytics adaptation is to develop the ability to measure clinical performance at the care team level and demonstrate its superiority in driving performance improvements and outcomes relative to existing organizational levels of aggregation, such as a hospital or medical group. The measurement should dovetail with the emerging reality that care, especially for the chronically ill, requires a well-functioning team of physicians, other caregivers, communities, and patients. The measurement might well influence the management of care to make the components work together for the good of the whole.
The analytic methods include predictive modeling, external data collection, integration, and dashboards. There are major challenges, including persistent resistance to performance measurement at a granular level and the belief that individual physicians are the key ingredient in producing patient outcomes. This might change the calculus about applying pay-for-performance incentives to teams rather than individual doctors.
Observations Across the Adaptations
There is a common thread running through six of the seven adaptations. Simply said, the way to improve outcomes is to ramp up the involvement of people in the co-production of their own health. There are many ways to improve health and healthcare and there are many stakeholders. But the sweet spots from other industries do not provide insights that emphasize how to dramatically improve operations (although banking is expert in its mastery of transactions processing), or how to improve clinical practice (although healthcare has drawn on industry techniques for quality control), or how to work with government (although banking does have painful experience with this).
What is obvious across the industries is the laser focus on customers, to win them over to buy certain products, to convince them to vote for certain candidates, or to excite them to come to the stadium to watch the game. As industries emerge from the Great Recession, the linchpin for innovation and the transformations needed to achieve profitable growth always center on the customer.
Not so in healthcare...for a variety of reasons, including perverse payment incentives, insurance, and the highly professionalized medicalization of the business, which favors a directive rather than a collaborative relationship with patients. As a result of these defining characteristics of the industry, there is a huge blind spot. Healthcare has not seen or valued the sophisticated advances developed in other industries to engage the customer. But the engagement needed in healthcare is not an easy translation from other industries; for example, to sell the product.
Healthcare actually needs to change the current way it sells services through the fee-for-service system because far too many services are pure waste. Healthcare needs a drastic reorientation to improve outcomes. If it embraces that idea, the most important contributor to achieving better outcomes resides with the individual, not the medical system, community systems, research advances, and everything else external to the individual. The one big idea healthcare can learn from other industries is to take care of the customer. Paradoxically, healthcare should have the best relationships with its customers because of the nature of the caring profession. But it has been resistant to fundamental ways to partner with people; for example, by truly making care patient-centric and by sharing decisions with patients on many issues that are just not medical and are mostly about the preferences and tradeoffs concerning one’s health.
The adaptations described in this chapter position analytics, in both simple and advanced forms, as potent catalysts to achieve these very important health goals.1