
Chapter 5
Leveraging Big Data Analytics for Personalized Elderly Care
Opportunities and Challenges
Obinna Anya1, and Hissam Tawfik2 1IBM Research – Almaden, San Jose, CA, USA 2Department of Mathematics and Computer Science, Liverpool Hope University, UK
E-mail: [email protected], [email protected]
E-mail: [email protected], [email protected]
Abstract
Owing to the growing increase in the world’s ageing population, research has focused on developing information and communication technology (ICT)–based services for personalized care, improved health, and quality social life for the elderly. Recent efforts explore Big Data in order to build mathematical models of personal behavior and lifestyle for analytics. Leveraging Big Data analytics holds enormous potential for solving some of the biggest and most intractable challenges in personalized elderly care through quantified modeling of a person’s lifestyle in a way that takes cognizance of their beliefs, values, and preferences, and connects to a history of events, things, and places around which they have progressively built their lives. However, the idea of discovering patterns to personalize care and inform critical health care decisions for the elderly is challenged as data grow exponentially in volume, become faster and increasingly unstructured, and are generated from sociodigital engagements that often may not accurately reflect the real-world entities and contexts they represent. As a result, the idea raises issues along several dimensions, including social, technical, and context-aware challenges. In this chapter, we present an overview of the state of the art in personalized elderly care, and explore the opportunities and inherent sociotechnical challenges in leveraging Big Data analytics to support elderly care and independent living. Based on this discussion, and arguing that analytics need to take account of the contexts that shape the generation and use of data, ACTVAGE, a context-aware lifestyle-oriented framework for personalized elderly care and independent living is proposed.
Keywords
Elderly care; personalized care; independent living; ACTVAGE; Big Data analytics; CAPIM; lifestyle-oriented; context-awareness; frameworkIntroduction
Advances in several subfields of information and communication technology (ICT), including social computing, sensor networks, the Internet of Things, and intelligent information processing, have given rise to “a world of data” [1] with fast and pervasive analytics at scale. In recent years, there has been a growing interest in collecting and analyzing data about several aspects of our life—our shopping habits and travel records, our “likes,” tweets, photos, digital clicks, and daily interactions and conversations with friends and family—via personal mobile devices, the social media, credit card swipes, wearable gadgets, smart buildings, intelligent vehicles, and advanced analytics applications. Although these pervasive data collection and analytics methods continue to grow and build digital profiles of us and our lifestyles, significant open questions remain as to what data should be collected, what insights should be drawn from them, and for what use.
Broadly speaking, one of such uses has been to support innovation and decision making, and one area where this has gained traction recently is the health care industry, particularly elderly care. Elderly people represent a growing proportion of the world’s population. As noted by the World Population Ageing Report [2], the population of people in the world aged 60 and older has risen from 205 million in 1950 to almost 810 million in 2012, and is projected to double by 2050, reaching 2 billion (approximately 20% of the world’s population and an increase of about 181% between 2010 and 2050). In addition, we are living longer. It is anticipated that we can expect to have an increase in life expectancy at birth from 86 years for males and 92 years for females by 2050 [3]. Building technologies to empower the elderly to stay healthy and active and, as importantly, participate in decisions pertaining to their health care is at the center of studies on personalized elderly care. Achieving this remains challenging primarily because of huge differences in individual care needs and the progressive nature of ageing [4].
Personalization entails processes that encourage and respect the contributions elderly persons can make to their own health—from the perspective of their values, goals, past experience, and knowledge of their own health needs—with the underlying goal of providing for them care that is “predictive, personalized, preventive and participatory” [5]. However, existing approaches often treat the elderly as compliant individuals, and deliver services through a series of discrete care episodes that hardly take account of the varied needs and lifestyles of the elderly [6]. With exabytes of data generated on a daily basis about our activities from digital footprints and online activities, recent research efforts are focusing on exploiting these massive data sets to address the challenge of personalized elderly care. But, despite the potential ability of Big Data to add to our knowledge of ourselves in novel ways and to enrich our understanding of people’s latent needs and preferences [7-9], deriving valuable insight from Big Data poses numerous challenges.
In this chapter, we describe the opportunities and challenges that leveraging Big Data analytics for elderly care presents. It is argued that though potentially viable as an approach to raise elderly care to a level where the uniqueness of each elderly person is adequately recognized [10], it does pose inherent and enormous social, context-aware, and technical challenges that research cannot afford to ignore. We present a review of research in personalized services for elderly care and explore the challenges in the area of Big Data analytics for elderly care. Based on the discussion, ACTVAGE—a context-aware lifestyle-oriented framework for supporting personalized elderly care and independent living is proposed. The framework combines systematic capture of past lifestyles and knowledge of current activities and user context. It then applies rigorous analytics to build a complete picture of the elderly person's lifestyle and contextual needs in order to build a formal representation of the lifestyle concept for system design. Based on the representation, required services, including social networking, self-diagnosis and monitoring, advisory, entertainment, exercise, dietary, reminder, and local events services are developed to offer individually tailored and lifestyle-oriented support for active ageing and independent living.
The Challenge of Personalization in Elderly Care
The notion of personalized care has been an important factor underlying the provision of quality care [11] and a central consideration in the design of health and social services for the elderly [10,12,13]. Personalized care places emphasis on the individual needs of a person rather than on efficiencies of the care provider or the sophistication of technologies for care support; builds upon the strengths of a person as an individual rather than on their weaknesses as a care receiver; and honors their values, personal choices, and preferences [12,14-16]. An overarching goal was to support the elderly care receiver to maintain a sense of self [10]. However, considerable confusion surrounds the notion of personalized care—what it means as a concept, what it involves in practice, and how best to take account of it in the design of computational systems for elderly care. More comprehensive discussions of the conceptual analysis and practical dimensions of personalized care are available [4,17-22]. The goal here is to highlight how personalization of care has become a particularly huge challenge as we develop more automated care services and ICT-based solutions to support the elderly [23,24].
• Difficulty in operationalizing the concept of personalization for system design: A review of the literature in health care indicates, as noted earlier, that there is lack of consensus about the exact meaning of personalized care. There is also considerable ambiguity to date concerning the optimum method of measuring the process and outcomes of personalized care [19,20,25,26]. One of the reasons for this, as Armstrong [27] noted, is that there is an inherent difficulty in choosing a single descriptor to qualify the “object” of care, that is, the person that clinicians and carers deal with on an everyday basis. The identity, and hence personality, of any individual is “both multi-faceted (biological, psychological, social) and ever-changing.” Elderly persons vary in their health and social care needs because they have unique circumstances and values and have different disease history and life experiences. They also vary in their personal wishes and desires, for example, preferred heating, lighting, exercise requirements, and audio levels. A key challenge becomes how to operationalize “personality” as a formal concept for system design to support the elderly through a care and treatment plan that recognizes the uniqueness of the individual and seeks to understand the world from the person’s perspective while supporting their psychological, clinical, and social needs [10]. Big Data analytics can help in abstracting key events in a person’s life so as to construct a computable account of their varying lifestyles and desires, especially for elderly persons with cognitive impairments.
• Technologies for elderly care often appear unduly technology-centric: The last decade or so has seen an explosion in technological innovation in the field of elderly care. However, adoption of technological solutions for elderly care does not appear to follow a similar growth trajectory [16,23,28]. As observed earlier, existing solutions often appear “fundamentally incompatible with ageing” [23] and deliver services through a series of technology-centric care episodes without consideration of the peculiar needs and preferences of the elderly, or what they can easily interact with [6,23,24]. In smart homes, for example, satisfying the needs of the user remains a major challenge in research and development [29]. Because of the huge focus on technology, as well as the speedy rate of advances in ICT, most technologies for everyday use are designed to last for a couple of years. For example, we change the way interfaces work, often for cosmetic reasons without recognizing that the elderly, with memory impairment, will find it difficult to adapt to such rate of change. Our industry faces the challenge of how to design full-function technology devices with a constant interface, for example, large easy-to-read screen displays, regardless of upgrades or new versions, that the elderly will find easier to use [23]. Second, the elderly often organize their homes for their particular comfort needs. As such, the introduction of technology into such environment needs to be nonintrusive, with minimal impact and without unduly effecting the elderly person’s interaction in that environment. Thus, any technology introduced must be adaptable to a wide range of environments and interactive behaviors as well as being as transparent as possible, for example, by adapting to personal lifestyles.
• Customizing and adapting technology design for optimum user satisfaction: Because ageing is a progressive process, technologies for elderly care need to keep track of developments in an elderly person, for example, new symptoms, in order to enable easy modification of care services [4]. As early as 1997 (when research in personalized computer support for the elderly was relatively gaining momentum), the French National Centre for Scientific Research–Science for Engineering consulted a group of experts on smart homes for the elderly to better identify research issues and define priorities (Estève [30] cited by [24]). The recommendations of the expert group, which have remained to a large extent a challenge to date, include allowing the elderly to express their values and choices, rather than outrightly treating them as compliant individuals, and to regard the elderly user’s surrounding, for example, activities, family, and neighbors, as important in the task of determining user needs. A key variable, therefore, in technology adoption by the elderly, and hence in ensuring that designs meet user needs, is the technology's perceived usefulness to the user [31]. As such, the design of technologies for elderly care should be driven by an understanding of actual need for the technology, ease of learning to use the technology, the elderly person’s cognitive and perceptual abilities, as well as other sociopsychological factors such as preferences, attitudes, beliefs, and involving the elderly user in the design process [28,31]. For the first time, the phenomenon of Big Data has provided us with cheap, large-scale data to ensure accurate understanding of the needs, beliefs, circumstances, and desires of the elderly person for system design. Using Big Data analytics, research can potentially build technologies that can relate new symptoms to an elderly person’s lifestyle and past habits, as well as medical history and genetic makeup, and even predict new symptoms before they occur.
• Building technologies that are dependable for elderly use: Given the vulnerability of the elderly, care services and technologies for their use need to operate in a predictable and dependable way [4] in order to guarantee the health and safety of the elderly users. Approaches in Big Data analytics, for example, quantified self, can help in generating accurate mathematical models of elderly users in a way that ensures that provided care services are robust, dependable, and exhibit desirable behaviors. As Big Data analytics evolves into a promising field for providing insight from very large data sets and improving outcomes, there is a need for a holistic approach that seeks not only to decipher who the elderly individual is [32] as the primary driver of care, but also to make the technologies usable for them.
Existing research approaches to developing personalized elderly care technologies can be broken down into two broad categories: (1) monitoring and surveillance, whereby electronic technologies are deployed to keep track of an elderly person’s medical condition and daily activities, and automatically alert health care staff when intervention is required. Research in this category focuses primarily on smart homes and the monitoring activities of daily living. (2) Assistive technologies, which can range from a simple device to help a physically impaired old adult, for example, with Parkinson disease to turn on a tap without much risk, to a personal robot that is able to spoon-feed an elderly person or administer medication without the need for a health care staff. In what follows, we briefly discuss a number of research efforts in these areas. These efforts overlap, and it is not unlikely to find, for example, a project that integrates the concept of a smart home and the technique of activities of daily living monitoring [33], or a smart home that employs a robot care assistant [29]. Our goal here is to critically review research in these areas in relation to the key challenges of personalized elderly care as discussed above.
Smart Homes
The smart home approach to personalized elderly care is one category of research in elderly care that has received a relatively high attention over the last decade or so, with many research and development projects ongoing and funded by international and governmental organizations. Examples of such projects include Life 2.0, OLDES, CAALYX, MATCH Home Care Project, and K4CARE.1 See [4,29,34,35] for a more thorough review of research in smart homes. The smart home offers a cost-effective way for caring for the elderly in “their own homes” without institutionalizing them and provides a viable solution to technology-driven assistive living for the elderly [13,33]. A smart home is “any living or working environment that has been carefully constructed to assist people in carrying out required activities” [29]. Research in smart homes has thrived in part because of a reliance on home automation systems, and the availability of supporting technologies, such as personal computers, sensors, passive and active electronic “tags,” and cellular phones. Existing works have concentrated on sensor networks, data collection and communication, and low-level ad hoc responsive assistance based on the simple processing of low-level raw sensor data using decision rules [33]. For example, if room temperature is below a specific value, start the air conditioner. Over the years, the task of building smart homes has integrated other approaches in health care for increased success. Telemedicine or “telehomecare”, for example, where clinical consultations and treatments are provided virtually to an elderly in a smart home via ICT technologies has been used for disease prevention and monitoring of the elderly [36]. Others include “the intelligent room,” which combines robotics, vision and speech technology, and agent-based architectures in order to provide computation and information services for people engaged in day-to-day activities with the goal of pulling the computer out into the real world of people [37]; “integrated home systems,” which provides for the elderly a single human–machine interface to household systems and gadgets [38,39]); “rehabilitation integrated systems” for better access and ergonomics for the elderly [40]; and the “adaptive house,” which uses advanced neural network to control such things as room temperature, heating, and lighting without previous programming by the residents [41]. Recent approaches leverage advances in context-awareness, for example, the context-sensitive rule-based architecture for a smart home environment [42]; social computing, for example, the aware community, which allows an elderly in a smart home to engage with other people via social networks [43] as well as mobile technologies, the service-oriented paradigm, and cloud-based infrastructures [44-46]. In addition, research in smart home has served as an environment for scientific study of home life, particularly the relationships between space and information, for example, through approaches that integrate learning into everyday activity in a smart home [44], in order to provide better personalized services for the elderly.
Despite the huge progress in smart home research, realizing the vision of smart home presents a number of challenges. Some of these challenges stem from the fact that at any specific time a smart home is required to generate data about the environment such as temperature and humidity; medication level; the status of doors, windows, and lights; and about the location and behaviors of its inhabitants, such as sleeping, cooking, watching TV, etc. As noted by [33], the central issue becomes how to fuse data from multiple sources in order to form a meaningful interpretation of a situation, in relation to other information sources such as electronic health records as well as information about user needs, and subsequently provide personalized care to the elderly inhabitant. A related challenge in smart homes is that the technologies often appear too intrusive and technologically too sophisticated and unusable for an elderly person [23]. Overall, existing smart homes hardly adapt to the personal lifestyles of the elderly.
Monitoring Activities of Daily Living
Monitoring of activities of daily living (ADLs), also known as lifestyle monitoring or behavioral monitoring, is an approach to elderly care where changes in activity profiles of an individual are used as a proxy to highlight a change in the individual’s health or care status [47]. Over the last decade, many studies on ADLs of elderly people have been carried out. For example, Gokalp and Clarke [48] present an excellent review of studies that monitored ADLs of elderly people; see also [49-51]. A key goal of ADL monitoring is to provide assisted living to the elderly person. Changes in daily activity level, including daily habits, movements, vital signs, etc. can provide important clues regarding functional ability, cognitive capability, loss of autonomy or independence, medication adherence, decline in health status, or progress of an existing illness, which could consequently be used as a basis to revise existing care plan [48]. Applications of ADL monitoring are based on four broad technologies: context-aware or ambient sensor technologies, tele-monitoring technologies, wearable technologies, and combinatorial technologies [48,49,52]. Most studies reviewed have focused on technologies and strategies for monitoring. The predominant monitoring strategy is that of detecting changes in activity levels of the elderly person, such as changes in motion or location, changes in body temperature or blood pressure, and the rate of access to the door or usage of appliances, for example, TV, refrigerator. Little attention was given to determining how changes in activity profile compare to the individual’s history of activity, or relate to the elderly person’s actual preferences. Brownsell et al. [47] outline a number of interesting research questions that still pose a challenge to research in ADL monitoring, which include determining the primary purpose and role of lifestyle monitoring (assessment or long-term monitoring, or both; providing effective monitoring of a person’s levels of activity using sensors; understanding sufficiently the link between health status and activity; identifying clearly the features of a particular person’s life and activities to be monitored; determining how analysis of ADL monitoring would be utilized in actual clinical services; and finally, identifying the requisite service response to monitoring, as well as the organizational and operational issues associated with monitoring. Although research in monitoring ADLs of the elderly appears quite promising, with many commercial lifestyle-monitoring products on the market, mostly for short-term health and care assessments,2 overall review suggests that monitoring ADLs remains relatively challenging, and there is little understanding about how to develop effective systems that would enable comprehensive care in a way that recognizes the individuality of an elderly person or seeks to understand the world from their own perspective.
Assistive Robot Technologies
Assistive robot technologies for elderly care have thrived largely as a result of growing advances in robotics and artificial intelligence and have led to personal robots that assist the elderly with daily tasks such as dressing and bathing, interact with them and provide companionship to ease the burden of loneliness, and even help them to communicate remotely with physicians and caregivers [3,29,53]. A number of research projects in this category combine the smart home concept (discussed earlier) with robotic assistance. They are rapidly advancing from engineering prototypes to potential commercial realities and positioned for mass market adoption. Examples include Hector, a mobile assistive robot for the elderly created out of the CompanionAble Project3 at the Intelligent Systems Research Laboratory, University of Reading, United Kingdom. Hector can work collaboratively with a smart home and remote control center to better support older people living at home, helping them stay independent for longer and avoid unplanned hospital admissions [3]. Other projects combine activity monitoring with robotics. For example, as part of an EU-funded research project, senior citizens in Italy, Spain, and Sweden have had their homes equipped with sensors to track their activity and health. Mobile telepresence robots, a wheeled videoconferencing system that can be piloted remotely, allow relatives and doctors check in with the elderly and interact with them [54].
There are two principal directions in robotics research (for elderly care), namely, task-oriented robotics and interaction-oriented robotics [55,56]. Task-oriented robots rely on physics and mechatronics to perform tasks in controlled specific environments. The most successful task-oriented robots serve in factory automation, where they typically assemble electronic devices or deal with heavy objects [56]. Task-oriented robots have been adapted for elderly care in smart homes, where they follow algorithms to perform well-defined tasks, such as alerting doctors and caregivers when medication has dropped below a certain level or when the elderly person has changed location within a smart home environment. Interaction-oriented robots, on the other hand, are designed to interact with elderly users and rely primarily on social behavioral theories. A central goal of research for the elderly was to explore important issues about what functions a robot assistant could provide to an elderly individual, as well as learning more about the way people interact with a robot when more “human-like” characteristics are introduced—many of which pose tremendous challenges from ethical and sociotechnical dimensions [57]. However, most work have been focused on technical testing of whether the technology does work, rather than on trying to understand how elderly people will choose to interact with the technology or have it adapted for them [29,33].
Big Data Analytics for Elderly Care
The goal of this chapter in discussing a review of challenges in personalized elderly care has been to show through such discussion why efforts to leverage Big Data analytics for elderly care should be tackled through a holistic approach that simultaneously takes into account the sociotechnical and context-aware challenges posed by personalized elderly care. As noted earlier, existing approaches to personalized elderly care, for example, smart homes, ADLs, and assistive robotics, appear overly technology-centric, lack a formal specification of the concept of personalization, and often treat the elderly as compliant individuals and deliver care services without sufficient consideration of the actual needs and preferences of the elderly, or their values and lifestyles. For the first time in human history, research has at its disposal zettabytes (1021 gigabytes) of data, that have been obtained from almost every fabric of our daily life activities—from hospital visits, travels, friends and family interactions, to occupational activities and shopping patterns—that could potentially be harnessed to gain a near perfect understanding of an elderly person’s lifestyles, values, beliefs, as well as a history of choices the person has made [58].
Big Data refers to data that are so diverse, complex, and large-scale combining both structured and unstructured information contents from multiple sources [59] so much that it is technically challenging, if not impossible, to be processed using existing traditional software and analytic methods, such as relational databases and management information systems. Boyd and Crawford [60] outline a definition that highlights so interestingly both the opportunities and challenges of Big Data in elderly care. According to the authors, Big Data is “a technological, cultural, and scholarly phenomenon” that rests on the interplay of three things, namely, (1) technology, taking advantage of increased computing power and algorithmic accuracy to gather, analyze, link, and compare large data sets; (2) analysis, drawing on large sets to identify patterns in order to make economic, social, technical, and legal claims; and (3) mythology, the computational turn in thought and research that large data sets offer a higher form of intelligence and knowledge that can generate insights that were previously impossible, with the aura of truth, objectivity, and accuracy. Data are not technically “neutral” [61], and if considered otherwise, become, in the words of Lisa Gitelman [62], an “oxymoron.” Deriving actionable value from Big Data, therefore, requires that research takes cognizance of the contexts that have shaped the data collection, the forms of arguments and analysis that can, and are, made with the data, as well as a clear indication of what the data do not, and cannot, account for [63]. Big Data4 for elderly care comes from three major sources. The first, popularly referred to as Big Data, involves analytics of multiple types of data across a population, typically over a period of time, potentially from multiple sources, of structured and unstructured nature, and of heterogeneous kinds of objects. This has been a by-product of ubiquitous smart technologies that have pervaded every aspect of our life. The second comes from what Cornell NYC Tech professor Deborah Estrin has called small data, the output of a whole host of pervasive tracking processes about any one individual, e.g. data from quantified self [61]. The third source of Big Data refers to what ethnographers, such as Tricia Wang [64], have called thick data, and includes more qualitative kinds of data, obtained, for example, from interviews and direct observational studies, which are needed to bridge and/or reveal knowledge gaps in quantitative and algorithmic Big Data. Besides the large volumes of data available to the health care industry, driven by digitization of EHRs, laboratory systems, physician notes, medical correspondence, regulatory requirements, and care plans [65-67], which many experts say double every five years, as well as data from social media and public health records, current approaches in the use of Big Data for elderly care tend to focus on the Big Data and small data categories. These approaches leverage ubiquitous sensor-enabled devices and such techniques as sociometeric badges [9] and the concept of quantified self5 [68]. Though potentially capable of providing statistical regularities in a “measured life” [69] and a mathematical explanation for understanding human dynamics [9] and personal health [70], these techniques have been critiqued for their tendency to hide rather than reveal the very essence of what makes us who we are [63], as they may automatically affect how “the self is understood, experienced, and practiced more broadly” [71].
The biggest opportunity that Big Data offers for the personalization of elderly care lies not only in the availability of large volumes of data but also in the diversity of both the types and sources of data. This opportunity, it could be argued, will potentially be harnessed at the confluence of health care and personal location data, which according to a recent report from McKinsey Institute, constitute two of the five domains that would be greatly transformed by Big Data [72]. As noted earlier, one of the major challenges in personalized elderly is the difficulty in specifying the concept of personalization and operationalizing it for computational design. This is all the more challenging in view of the fact that elderly people usually suffer multiple age-related ailments, such as dementia and Parkinson disease, that impair considerably their cognitive and physical capabilities. In such cases, health care practitioners often resort to information from historical records and family members in order to gain an understanding of the patient. By digitizing, combining, and effectively using Big Data, the health care industry stands an unprecedented chance to gain a significant understanding of the elderly patient. This will lead to more targeted treatment outcomes and increase the chances of detecting diseases at earlier stages when they can be treated more easily and effectively. In addition, certain care outcomes, such as allergies, risks of infection or hospital-acquired illness; or the possibility of identifying patients who may choose elective surgery or benefit from proactive care or lifestyle changes; or the possibility of comorbid conditions due to environmental, family, or lifestyle factors, etc. can be more effectively estimated on the basis of historical data [13]. Big Data is deeply related to the phenomenon of e-Science [73], computationally intensive science that is usually carried out in highly distributed computing environments, using immense data sets and requiring grid computing. From this perspective, Big Data will potentially play a vital role as a part of e-Social Science in collecting, processing, and analyzing social and behavioral data [74] for personalized elderly care.
Requirements and Challenges for Big Data–Driven Elderly Care Applications
Creating value from Big Data requires a holistic understanding of the nature of data in Big Data that gives rise to issues of variety or heterogeneity of data, incompleteness and inconsistency, timeliness, privacy, context, collaboration, and visualization, as well as challenges that arise as a result of the multistep processes in Big Data analytics and the tools ecosystem around Big Data [75]. Big Data in health care and elsewhere is characterized by five V’s that constitute the five key dimensional challenges in Big Data analytics, namely, volume, velocity, variety, veracity, and value.6 These pose nontrivial challenges in elderly care just as they do in other areas where Big Data analytics is being explored as a potential solution, for example, health care [66,76,77] and smart city [78]. Already, one of the greatest problems to the deployment of Big Data analytics in care is deciding what data is relevant [76]. As new forms of Big Data for elderly care, for example, QS, sociometric monitoring, and genome sequencing, begin to fuel this exponential growth, the problem of finding the needle in the haystack becomes significantly worse [75,77]. A downside of the growing size of Big Data, which presents a challenge to analytics, is that in most cases, for example in health care, up to 90% of the data generated are discarded [77]. Fortunately, advances in data provisioning and data management, such as cloud computing and virtualization, are facilitating the development of platforms for more effective capture and storage of large volumes of data on demand [79].
An associated challenge is the constant flow of new data streaming at unprecedented rates. Velocity of data increases as data are accumulated via various real-time devices, such as daily monitoring of glucose level in diabetic patients, QS, blood pressure reading, etc. Many systems for streaming data often perform the same functions; meaning that data must be rationalized and normalized, which adds to the analytics overhead. Similarly, because a wide range of systems are deployed for Big Data capture, data often come in enormous variety—structured, unstructured, and semistructured—a dimension that is both interesting and challenging to elderly care. The variety of data from multiple sources may define data values differently, thus increasing complexity and inconsistency of data. For example, only relatively small percentage of data streams about our daily activities, for example, from fitness devices, genetics, travel records, genomics, social media, and other sources can presently be organized and analyzed for meaningful and actionable insight [77]. Elderly care applications need more efficient and automatic ways of converting and combining varieties of data from multiple sources in order to enhance data relevancy and create value for personalized care.
Of the five-dimensional V's of Big Data, veracity is perhaps the most difficult to quantify, verify, and measure. Veracity or “data assurance” becomes arguably a critical issue because of the increase in the use of nonscientific methods and practices in Big Data gathering. Data without veracity creates vulnerability, and affects adversely the validity and reliability of analytics results. In a survey by IBM, about 30% of respondents expressed concern that as data currently stand, it is hard to know which information is accurate and which is out of date. One in three business leaders do not trust the information they use to make decisions. What’s more, poor data quality costs the U.S. economy around $3.1 trillion each year, providing a huge incentive for the development of tools and systems that maintain the veracity of data [80]. Data quality issues are of acute concern in elderly care, as the use of inaccurate information at the point of care could be fatal. More research is needed to develop algorithms with the capability to understand poor heterogeneous data, for example, by automatically generating the right metadata to describe the recorded data.
Value, of course, is the goal of Big Data analytics. Developing an effective means of addressing the challenges posed by volume, velocity, variety, and veracity will ultimately lead to high data value and more useful insights for elderly care. Equally important is the need for analytics to place significant importance to every step in Big Data analytics, and developing tools to support them. Many studies show that out of the multiple steps of Big Data analytics, namely data acquisition, extraction and cleaning, integration, modeling and analysis, interpretation, and deployment, much research attention has focused on one or two steps, ignoring the rest [75]. Current approaches for extracting value from Big Data are varied, ad hoc, and highly application-dependent [81]. Other requirements and concerns in Big Data analytics, for example, privacy, data ownership, usability, choice of analytics platforms, architectural design, support for efficient data storage and real-time guarantees, virtualization requirements, and the dominance of the open source paradigm remain and have been variously addressed in the literature (see e.g. [75,77,81,82]). For example, although many countries and health care organizations have developed laws governing how data can be used and revealed in different contexts and for different purposes, there is still huge public concern about the inappropriate use of personal data, particularly through linking of data from multiple sources [75]. Privacy, like most of the other concerns discussed above, is both a technical and a sociological problem and can only be effectively addressed from both perspectives. However, the five V’s represent an appropriate starting point for a discussion about the challenges of Big Data analytics for personalized elderly care.
The Role of Context
Like many health care applications for personalized support [49] and intelligent services [78], elderly care systems are highly dependent on their execution context. A common definition of context considers it as “any information that can be used to characterize the situation of an entity,” where an entity refers to a person, place, or object that is considered relevant in an interaction sequence [83]. Context is critical in the design of care support systems for the elderly because of its ability to enable us to construct and maintain awareness of a person’s activities, status, or context in different settings, yet it has remained a poor source of information in computing environments [83]. As a result, the term has been considered differently by different authors—as the surroundings of the interaction between the user and the application [84], what is needed to characterize and encode the situation of an entity [85], information about the activity or task the user is currently performing [86], or what is needed to understand what people do, and how and why they achieve and maintain a mutual understanding of the context for their actions [87].
In Big Data analytics, context provides a structure to ensure that discovery of patterns and relations from Big Data occur within the right contextual setting, which Sokol and Ames [88] refer to as situational awareness. By using situational data to gain knowledge of the complex and dynamic environments in which humans perform their tasks and adding a rich and correct cumulative context to Big Data analytics, analytic model accuracy is greatly enhanced. Context can provide metadata for making sense of Big Data and for addressing such concerns as privacy and consistency by offering a description of the entities that are relevant to a set of data—people, organizations, and relationships between the entities and events [88]. Dobre and Xhafa [78] outline a number of requirements for designing context-aware support in Big Data analytics applications, which include providing real-time guarantees for data provisioning, helping users augment their reality by providing information about mobility and locality, providing support communication and connectivity imperfection, and providing support for efficient data access, storage, and analytic scalability.
Proposed Framework
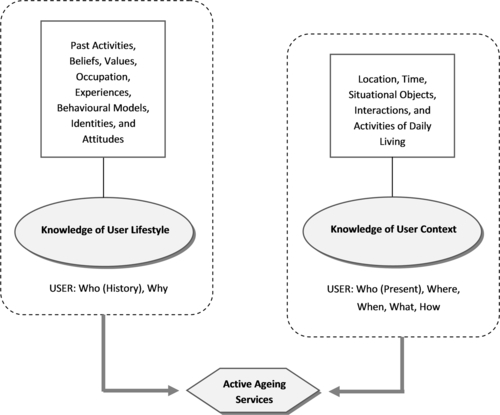
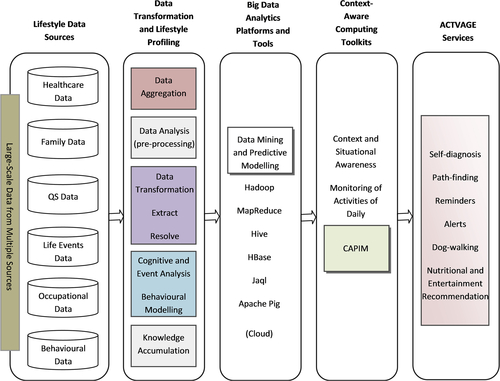
Although research in personalized elderly care has not so far sufficiently addressed all the fundamental challenges of personalization in elderly care, a number of important successful results have been obtained, particularly in the area of context-aware support in monitoring and surveillance in smart homes and the development of situation-aware assistive technologies [49,50]. Leveraging the trend of research on context-aware user support, particularly the works of [85-87,89] and building on the unique capabilities of Big Data analytics in amassing and analyzing large-scale data about individual behaviors and lifestyles (as discussed earlier), we present in this section the conceptual framework of ACTVAGE, a context-aware lifestyle-oriented framework for supporting personalized elderly care and independent living. As shown in Figure 5.1, the proposed framework combines an understanding of user lifestyles, personal preferences and beliefs, as well as knowledge of user context in order to offer a model of ICT-enabled support for independent living.
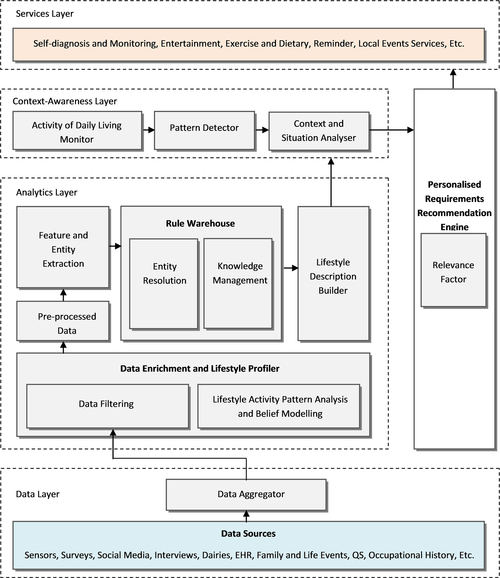
The framework consists of four layers, namely, the data layer, the analytics layer, the context-awareness layer, and the services layer (see Figure 5.2). The approach will combine systematic data capture and rigorous analytics to uncover the actual and complete picture of the elderly person's lifestyles and build a formal representation of the lifestyle concept for system design. Lifestyle information is integrated with context-aware capabilities that are dynamically configurable using the user’s location, identity, time, and an understanding of user activities of daily living in order to provide personalized recommendations. Based on the recommendations, a set of active ageing services are developed, using the capabilities of mobile devices and cloud-based services, to offer individually tailored and lifestyle-oriented services for active ageing and independent living, including social networking, self-diagnosis and monitoring, advisory, entertainment, exercise and dietary, reminder and local events services. The e-services will leverage on advances in ICT, including pervasive computing and usability engineering, for the provisioning of rich and platform independent e-services.
In developing the conceptual design of ACTVAGE, we draw on the seven principles and best practices to guide the development of Big Data analytics systems [74,90,85]. Exploiting Big Data analytics, as noted by Chen and Zhang [74], requires not only new technologies but also new ways of thinking. In the remainder of this section, we describe the steps and activities of the proposed framework and illustrate its application.
Step One: Data Aggregation and Processing
The main tasks in this step include aggregating, filtering, and preprocessing data from large volumes and different sources that “informally” describes an individual's lifestyles. Later, the data is formalized in order to transform it into a formal model for the design of e-services. Various approaches for human-centered computing [91], for example, contextual inquiry, ethnography, and experience sampling, as well as some analytics-driven approaches such as QS and sociometric monitoring, will be employed bringing together elderly persons, health care staff, families, and communities to explore and understand the real-life experiences of using health care technologies for independent living and to elicit the actual needs and requirements for the design of active ageing services for personalized elderly care. Formal techniques for requirements gathering, including questionnaires, interviews as well as profiling and personas will be employed with a focus on specifically making the ACTVAGE system usable.
Step Two: Lifestyle Modeling and Formalization
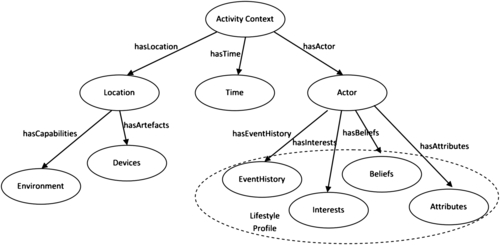
In this step, the data captured from the previous stage will be formalized in order to transform it into a formal model for the design of active ageing services. This stage will involve the use of modeling and simulation tools, including rule-based systems, as well as cognitive methods and the specification of a lifestyle ontology to enable proper representation of the lifestyle concept. The lifestyle ontology will be integrated with a context ontology for the creation of person-centered and context-aware e-services for the elderly patient that enables quality and independent living. Figure 5.3 shows an activity context model for building a context ontology. The hierarchical context model draws upon the CAPIM context [89], and aggregates the information—location, time, actor—necessary to detect the relevant attributes of a past activity into a unique set of data. In the model, we use the term actor to represent an elderly person or user to be supported. Information about the actor’s history of events, social interests, beliefs, and personal attributes is used as context information in building the actor’s lifestyle profile. Lifestyle profile will be implemented as lifestyle graph, where vertices represent life events, and edges represent relationships between life events. The vertices will consist of two types of life events: atomic events and composite events. Composite events are derived from atomic events. An example composite event in an actor’s event history would be “attend Liverpool Community College.” Multiple atomic events included in this composite event would include things the person did while at Liverpool Community College, for example, “was a chorister.” The process of lifestyle modeling and formalization will draw on research in life event modeling (e.g., [92,93]) and will include computer-based knowledge representation formalisms such as (1) a behavior-aware and lifestyle ontology and (2) a lifestyle description language. The resultant computer-processable representation will be integrated with context ontology in order to provide a richer description of an elderly person's lifestyle, situations, and preferences for the development of a lifestyle-oriented e-services framework.
A key feature of this step is the use of behavioral and neurophysiological measures, as well as the formalization of the lifestyle concept using primarily cognitive methods, event modeling, and data mining, and activity pattern analysis. It involves the use of rule-based systems, agent-based modeling, as well as the specification of a lifestyle ontology to enable proper representation of the lifestyle concept. The use modeling would enable the creation of generic care and support workflows for elderly care. The integration of the lifestyle ontology with a context ontology allows for the creation of person-centered and context-aware e-services for the elderly patient that enables quality and independent living. A central goal here is to enable the transformation of the data acquired in step one into a formal model of user lifestyle for the design of active ageing e-services
Step Three: Lifestyle-Oriented Context-Aware Recommendation
The next step of our approach is to add information about the user’s current activities, location, time, etc. as context variables to the formal lifestyle model developed in the previous step (Figure 5.4). This step will be implemented using CAPIM, a context-aware computing platform developed by [89]. CAPIM includes services that are able to aggregate and semantically organize context data. The services react based on dynamically defined context-oriented workflows, such as those specified in elderly care plans and captured from monitoring activities of daily living. The platform includes an execution engine that supports context-aware actions for orientation, information, and recommendation. A key advantage of CAPIM is that it actively and autonomously adapts and provides the appropriate services or content to the user, using the advantages of contextual information without too much user interaction [78]. Enabling efficient mechanisms for provisioning context-sensitive data to users is an important challenge in these types of context-aware platforms, whereas provisioning context services in a nonintrusive manner remains a major advantage.
Step Four: Active Ageing Services Composition
This step will involve the development of lifestyle-oriented context-aware services that provide “back-end” behavior to be integrated into ACTVAGE prototype. These services will have the capability to monitor and influence user behavior and support independent living in line with personalized profile models defined during lifestyle profiling, as well as context information generated in step three. The development of these services will follow a traditional waterfall-type development lifecycle, and will involve two iterations of the following tasks: (1) interpretation and analysis of requirements (initially from the lifestyle profiling stage, and from testing/validation feedback on the second iteration); (2) identification of input, output, and processing requirements; (3) specification of software-level interfaces, and design of methodologies/algorithmic approaches that can achieve the requisite behavior; (4) implementation of a set of software services that underpin “active ageing” functionality in the ACTVAGE platform; and (5) testing of developed services against the lifestyle profiling stage requirements, live user requirements, and feedback to beta phase.
Although the lifestyle profiling stage will provide significant detail and design guidance in terms of the lifestyle description language and surrounding vocabulary; initially, the developed services are categorized as follows: (1) critical and/or monitoring services, (2) social networking or communications services, and (3) exercise/activity, dietary, and behavioral services. They will utilize the concepts and behaviors determined and formalized in the lifestyle profiling stage to provide customized lifestyle-oriented services for active ageing, using the architectural design and tools in Figure 5.5. In implementing the ACTVAGE services, emphasis will be placed on assessing how well and seamlessly the services integrate with typical home appliances that the elderly persons are accustomed to for consistency in system interfaces.
Example Scenario
In order to demonstrate the applicability of our proposed framework, we illustrate using a hypothetical example of a dementia resident how ACTVAGE could be used in a real-world setting. Dementia is a condition related to ageing, with symptoms ranging from memory loss to decreased reasoning and communication skills [10]. As of 2010, the number of people with dementia was estimated at 35.6 million worldwide, and the number is expected to double every 20 years [94].
It is usually the norm that people with dementia, especially in rich economies where attaining great age is increasingly the case, are cared for in residential homes by professional (though not highly paid) carers whose job is typically viewed as having low status [10]. They are usually under pressure to balance work and administrative duties and are left with little time to gain sufficient understanding of their residents. In addition, these carers regularly encounter challenging behavior from the residents, including refusal to eat and take medication, inconsistent behaviors, and physical and verbal aggression that is difficult to diagnose and resolve [10]. No two residents are alike, and what has worked for one might not work for another. Existing solutions have leveraged techniques in person-centered care. However, there remains the need to gain an in-depth understanding of a dementia resident, particularly in cases where families do not have much valuable information about the resident. Here, we discuss how the various steps in ACTVAGE could enable a carer gain an in-depth understanding of a dementia resident’s life history, values, and interests for personalized care (see Figure 5.6).
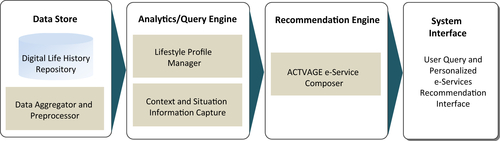
The system acquires data using both Big Data and thin data driven approaches (Facebook and Twitter data) as well as thin based approaches (semistructured interviews) via the Data Aggregator (see Figure 5.4). The data sets acquired are preprocessed, transformed, and stored in the digital life history repository. As shown in Figure 5.5, the repository contains data about several aspects of a resident’s past life events, interests, values, and preferences—modeled as a lifestyle graph (in step two). The Aggregator is designed to allow the carer and family members to remotely upload information about a resident using separate bespoke mobile apps and web applications, such as Digital Life Story.7 Context information about user activity is captured via wall-mounted cameras. The carer is able to enter queries and perform data analysis aimed to construct user lifestyle profile using the analytics and query engine. Services are composed in the recommendation engine. The system interface allows the carer to perform these actions as well as to view and analyze system output.
Discussion and Conclusion
The power to generate continuously growing amounts of data, scaling up to unprecedented volumes and streaming in different varieties and at fast rates presents a unique opportunity to address the problem of personalized elderly care by enabling us to construct data-driven mathematical models of individual persons for analytics. This capability is made possible primarily by two factors. First, technologies for readily collecting vast amounts of data are becoming available in more and more application areas. Second, infrastructures for persistently storing these data and processing them are becoming a reality. Interestingly, this power has become available at a point in human history when the world is facing a growing increase in its ageing population [2]. However, Big Data analytics equally brings several challenges to data processing and analysis. The features that define Big Data, such as volume, velocity, veracity, etc., and the multistep processes required to derive value from Big Data demand new processing and storage algorithms that go beyond what existing database and information processing systems offer. In addition, they pose system design and nontechnical challenges along several dimensions including sociological and context-awareness issues.
This chapter contributes to research efforts that aim to highlight the opportunities and challenges of Big Data analytics and lay out foundations for the design and development of applications that leverage the Big Data to address the problem of the world’s ageing population. We present an overview of research in personalized elderly care, and explore the opportunities and challenges in leveraging Big Data analytics for personalized elderly care and independent living. In particular, we have focused our discussion of the opportunities and challenges to be addressed in relation to the five-dimensional V’s of Big Data, as well as the multistep process of Big Data analytics, while acknowledging that other challenges remain that are not covered in this chapter. Based on this discussion, we propose ACTVAGE—a context-aware lifestyle-oriented framework for supporting personalized elderly care and independent living. The framework will potentially improve elderly care through the development of a model of ICT-enabled support for independent living that is grounded in an understanding of a history of user lifestyles and personal preferences, as well as knowledge of user activity context. By developing a set of lifestyle-oriented active ageing e-services, the proposed framework makes a novel contribution to elderly health care through an approach that exploits the lifestyle concept combined with context-aware user support, which itself has received considerable attention in ICT and computer science research, as a foundation for informing the design of ICT-enabled active ageing services and products. In addition, the approach will lead to the development of usable technologies for encouraging independent living, reducing reliance on institutionalized care, and promoting active social and healthy life into old age.
In a compelling paper, Choudhury et al. [95] present an approach that leverages Big Data, in particular Facebook data, to identify women at risk of postpartum depression at an early stage and provide them access to appropriate services and support. They employed statistical analysis and survey techniques to demonstrate the feasibility of Big Data as a tool to detect, characterize, and predict postpartum depression in new mothers, and as a result, recommend treatment plans to avoid recurrence. Like Choudhury and her colleagues, this chapter makes a case that Big Data has the potential to revolutionize care by providing us access to the vast amounts of data about individuals via self-reports, transaction data, and online activities as ground truth for developing ICT-based services for health care. We propose this innovative approach in a way that integrates digital life history with user activity context.
The chapter has focused on a high-level description of the ACTVAGE framework and lacks specific details about a number of the techniques included in the proposed framework, for example, life event modeling, ontology development, graph analytics, context information processing, and service composition. Future work will focus on developing specific details of the framework as well as prototype and evaluate systems based on it within a real-world application context. Our goal here is primarily to present the conceptual architecture of a new framework that combines knowledge of user lifestyle and knowledge of user activity context toward tackling the problem of personalized elderly care, and to show how the conceptualization was informed by meta-analysis of studies in personalized elderly care. As such, we have pointed to research studies, tools, and techniques that could be leveraged in developing and implementing solutions based on the proposed framework. In addition, we have illustrated the applicability of the framework to support elderly people living with dementia using a real-world example scenario. Integrating context and history of lifestyles into a single framework presents a lot of challenges. The value to be derived from Big Data is both analytically and technically bound to the context of production and use of the data, which as Dourish [87] notes is “a slippery notion” [p. 29]. Context is a central issue for Big Data analytics system. The power of Big Data to deliver on the promise of differentiated and useful insights lies precisely in the ability of analytics algorithms and systems to take into account both the context that has shaped data production and the context within which analytics-driven recommendations would be utilized. The overarching goal of the work described in this chapter is to lay a foundation for combining Big Data analytics with context-aware computing as a novel way to address the problem of personalized elderly care. The proposed framework will equally apply to many problem areas that leverage Big Data analytics.
..................Content has been hidden....................
You can't read the all page of ebook, please click here login for view all page.