
Chapter 10
Sociocultural and Technological Barriers Across all Phases of Implementation for Mobile Health in Developing Countries
Yvonne O’ Connor1, Siobhan O’ Connor2, Ciara Heavin1, Joe Gallagher3, and John O’ Donoghue4 1Health Information Systems Research Centre, University College Cork, Ireland 2School of Nursing, Midwifery & Social Work, University of Manchester, UK 3Health Research Group, University College Dublin, Ireland 4Global eHealth Unit, Department of Primary Care and Public Health, Imperial College London, UK
E-mail: [email protected], [email protected], [email protected], [email protected], [email protected]
E-mail: [email protected], [email protected], [email protected], [email protected], [email protected]
Abstract
In recent years, scholars are realizing the importance of examining mobile health (mHealth) implementation in developing countries. A vast array of research exists that focuses on barriers of mHealth adoption in such domains. However, the majority of these papers embrace the concept of adoption to cover the entire process of implementation. This chapter acknowledges that various phases of implementation exist. As a result, the researchers identify potential barriers for each phase of mHealth implementation in developing countries. By examining extant literature, this study reveals that various sociocultural and technological factors across individuals and organizations collectively can hinder mHealth implementation in developing regions. Extant research indicates that the focus of mHealth in these constituencies, a nascent area of research, places too much emphasis on the benefits associated with mHealth implementation. Subsequently, this chapter endeavors to outline the barriers that should assist with overcoming common obstacles in the successful implementation of mHealth initiatives in developing countries.
Keywords
Barriers; Developing Countries; Mobile Health; mHealth; Implementation; Sociocultural; TechnologicalIntroduction
The advent of mobile information technology (IT) has brought about profound opportunities in terms of their organizational application [1] by introducing new flexibility in terms of when, where, and how these technologies can be applied [2]. In the last decade, the application of mobile IT within health care, referred to as mobile Health or mHealth [3], has revolutionized the delivery of health care services [4]. The last decade witnessed a multitude of mHealth initiatives being deployed worldwide, with reports of more than 100,000 applications currently available to a variety of users [5]. mHealth offers a range of opportunities to its end users, from greater patient empowerment to improved clinical decision making, disease surveillance and monitoring, behavioral change and self-monitoring [5], to name but a few. With the documented evidence of numerous benefits and positive health-related outcomes associated with mHealth initiatives, many new mHealth projects are becoming ever more commonplace in developing regions [6]. mHealth is considered an appropriate avenue for delivering health care services, as the health care infrastructure and services are often insufficient in developing countries [7]. The unique characteristics of mHealth (e.g., ability of health workers and patients to communicate over vast distances) help improve the existing underresourced health infrastructures, ultimately translating into benefits for patients [8]. However, it is reported that some mHealth projects have failed (as depicted later in this chapter). Failure is defined as an infrequent, inappropriate, and ineffective long-term use of mHealth technologies [9]. As a result, this chapter’s primary focus is on identifying barriers to mHealth technology implementation in an effort to understand why some mHealth initiatives fail. To understand this phenomenon, the IT implementation process is subsequently described.
Mobile Health Implementation
Implementation of IT is defined as “an organisational effort directed toward diffusing appropriate information technology within a user community” [10]. Prescott and Conger [11] argue that some studies embrace the concept of “adoption” to cover the entire process of implementation. However, research exists which demonstrates that implementing IT is performed over several phases. In 1990, Cooper and Zmud [12] presented a detailed overview of the implementation phases for IT. They proposed that IT implementation consisted of six phases, namely, (1) initiation, (2) adoption, (3) adaptation, (4) acceptance, (5) routinization, and (6) infusion. Each phase is described in Table 10.1 as per Cooper and Zmud [12].
Although numerous implementation models exist in the literature [13-14] the researchers employ the Cooper and Zmud model [12] of IT implementation for three reasons: (1) the model is one of the most comprehensive models in literature for exploring IT implementation; (2) each phase is clearly defined, making it easier for examination purposes; and (3) the definition of IT implementation adopted for this study coincides with the definition proposed by Cooper and Zmud [12]. Employing a theoretical lens following Cooper and Zmud’s [12] technological diffusion model will enable the researchers to gain better insights into mHealth implementation processes within a developing world context. Implementation of any IT solution is usually a costly and difficult process [15]. In developing countries, the implementation process is often more challenging due to economic, demographic, and environmental factors [16]. Yet there exists a dearth of research that focuses on mHealth technology implementation in developing countries. Moreover, extant research is criticized for embracing the concept of adoption to cover the entire process of implementation although numerous phases exist. This chapter seeks to address this gap in extant literature by identifying key barriers to mHealth implementation, vis-à-vis a literature review, using the Cooper and Zmud [12] model as a baseline reference.
Table 10.1
Description of Phases in Technological Diffusion Model
| Phase | Description |
| Initiation | Scanning of organizational opportunities with mHealth technologies |
| Adoption | Negotiations to achieve organizational backing |
| Adaptation | Development, installation, and maintenance of new mHealth technology |
| Acceptance | Organizational members are induced to commit to using the new mHealth technology |
| Routinization | Organization’s consideration of the new mHealth technology as a normal activity |
| Infusion | Integration of new mHealth technology with the organization’s system to support higher levels of individual/organizational work |
Adapted from Cooper and Zmud [12]
Methodology
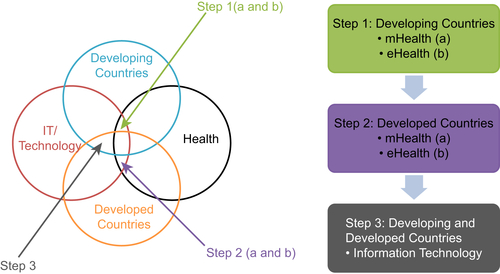
A literature review across a number of domains was performed. The selection strategy employed to identify the primary, secondary, and tertiary literature is illustrated in Figure 10.1.
This nascent research area relies on a significant body of interdisciplinary scholarship [17] that encompasses IT/technology, health, developing countries, eHealth, and mHealth literature (Figure 10.1). In order to fully pursue the concept of mHealth implementation in developing countries, the authors had to move beyond the primary literature to provide comprehensive coverage of the topic under investigation. First, mHealth in developing countries research was reviewed and examples are provided in subsequent sections (Step 1a in Figure 10.1). When this search revealed no documented examples, as per Cooper and Zmud [12] implementation phase definition, the authors reviewed the eHealth literature in developing countries (Step 1b in Figure 10.1). In reviewing later implementation phases, it became apparent that little evidence on mHealth and eHealth research in developing countries exist, which required the authors to view potential barriers initially from a developed country (Step 2a and b in Figure 10.1) and a wider IT perspective (Step 3 in Figure 10.1). This is due to the fact that the vast majority of mHealth initiatives deployed in developing countries are pilot studies and have not yet reached large-scale nationwide implementation [8]. The authors acknowledge that it will take some time to reach a level of maturity of mHealth in developing countries.
Potential Barriers to mHealth Implementation in Developing Countries
This section identifies various barriers that could hinder individual phases of implementation. According to Norris et al. [18], “frequently, public health interventions and campaigns have limited success because they emphasise the need for change when none is apparent and they fail to raise personal awareness.” This section comprises seven subsections, six of which are structured based on the Cooper and Zmud model presented in the second section of this chapter, while the seventh subsection summarizes the findings.
Potential Barriers to mHealth Initiation
As the name suggests, the initiation phase is the first phase of implementation according to the Cooper and Zmud model [12]. During this phase, active and/or passive scanning of organizational problems/opportunities and IT solutions are undertaken. That implies seeking new technological innovations to assist organizations in achieving their goals and/or address existing problems. From reviewing and synthesizing the literature, the following barriers have been identified that impact the initiation process of mobile IT, namely, lack of market competition, lack of awareness, and switching costs.
Market Uncertainty
It is deduced from the work of Mansfield et al [19] that market uncertainty can diminish the possible introduction of technological innovations into organizations. In 1986, Robertson and Gatignon [20] argued that the motivation to recognize new technology stems from the external market. This point is further reinforced by Funk and Methe [21], who found that market uncertainty can impact an organization’s decision to employ technological innovations. However, because of economic hardship faced by organizations in developing countries, the introduction of mHealth onto the marketplace has been limited. Many of the mHealth projects explored in development countries are funded and transferred from western societies, primarily on a pilot study basis [22,23].
Lack of Awareness
One of the major obstacles faced by users in resource-poor settings is their unawareness of the opportunities mobile technologies may provide in their location. This unfamiliarity with potential mobile technological resources is a counterproductive factor when seeking new technological resources, as information is required to facilitate decision making and stimulate progress to ensure existing practices can be improved upon. This inexperience or unawareness of the benefits of using mobile IT to solve organizational problems and/or increase opportunities therefore goes unnoticed. As such, lack of awareness hinders mobile IT implementation at the initiation phase.
Switching Costs
With various competing priorities for a dwindling financial resource, organizations in developing countries are often compelled to examine the criticality of investing in potential products. When deciding to invest in mHealth, users may switch from using one technological innovation to another, or substituting vendors (commonly referred to as “switching costs”). Borrowing and adapting the work of Kim and Gupta [24], this study defines switching costs as an organization/individual’s subjective perception of disutility (e.g., time, effort, economic resources, and emotional discomfort) associated with the process of switching from one vendor to another. In developing countries, the luxury and opportunities of switching technologies is not feasible because of economic constraints in such environments. In general, initial investments already devoted to existing technologies in the organization/individual’s current situation may discourage customers from switching to new mobile IT [25]. As a result, switching costs are likely to play a substantive role as a barrier to mobile IT initiation.
Politics
It is reported that internal politics can also have a major influence on the direction and depth of technological advancements within a given context [26]. In his work, Ziaie identified a number of impediments to IT implementation in a developing country (Iran) based on political or ideological reasons, including, sanctions, lack of support from highest political bodies, and unfamiliarity of higher authorities with IT-related complications. Kalathil [27] argues that information transparency that can be facilitated by IT may threaten decision makers in developing countries where corruption is more prevalent. Without sufficient governmental support, mHealth initiatives are less likely to succeed.
Potential Barriers to mHealth Adoption
The adoption phase of the Cooper and Zmud [12] model is the second stage of implementation, whereby the primary focus is on negotiations to achieve organizational backing. To achieve this, it is important that a decision is attained to invest resources necessary to accommodate the implementation effort. Indeed, Chib [28] contends that the nascent stage of mHealth adoption has resulted in an overstatement of its associated benefits. A review of the literature revealed that this process encounters a number of barriers, namely, insufficient readiness/resources, lack of supporting policy, and social influence/contextual barriers.
Insufficient Resources
It is reported that the majority of mHealth initiatives in developing countries are funded by external benefactors and are not self-sustaining, thereby affecting long-term sustainability of such projects [29]. It is imperative that resources and support are available when implementing IT applications. Without sufficient resources, mHealth solutions are destined to fail, as experienced by Medhi et al. [30] and Matheson et al. [31]. Both researcher groups witnessed drawbacks to using mHealth solutions due to insufficient technical support and funding difficulties, respectively.
Lack of Supporting Policy/Legal Issues
Policy pertaining to mHealth can be defined as “a set of statements, directives, regulations, laws, and judicial interpretations that direct and manage the life cycle of mHealth” [32]. The use of mHealth approaches within or between institutions involves several factors that require proper planning, supported by well-defined policies at the institutional, jurisdictional, and global levels. The absence and variety of these policies may lead to inadvertent widening of gaps in health status and knowledge levels between different sectors of the population, and increase rather than decrease health inequity. A systematic review of policy issues within the eHealth domain found 99 different policy issues, which could be grouped into nine categories [33]. Recent WHO analysis indicates a lack of knowledge about available mHealth applications and public health outcomes and absence of supportive policies at the country or regional level [34]. Low- and middle-income countries struggle to develop and implement policy and legal solutions in a rapidly changing field given their constrained resources.
Social Influence/Contextual Factors
Social influence is complex in nature and may be viewed from three perspectives: (1) compliance, (2) identification, and (3) internalization, all of which can be affected by a number of contextual factors, including limited resources and lack of expertise [35]. As outlined in O’ Connor et al. [36], a person’s intention to adopt a new mHealth technology is directly related to a number of contextual factors in association with the individual’s value system, which is heavily influenced by social values among others. This is an important note, in that mHealth solutions that may be acceptable within a developed country setting may not directly translate successfully to a developing countries environment unless the individual’s value system, which includes social influence, is correctly taken into account. Social influence should not be seen as an independent or standalone construct when looking at adoption [37,38]; therefore, a more holistic viewpoint should be considered to help ensure overall adoption.
Potential Barriers to mHealth Adaptation
Adaptation is the third phase of IT implementation as outlined in Cooper and Zmud's model [12]. This encompasses the development, installation, and maintenance of the IT application in the organization. A review of the literature revealed that this process encounters a number of barriers that can impact the adaptation phase of mHealth implementation, namely, language barrier, lack of training, poor availability of mHealth technologies, poor technical infrastructure, and issues regarding security and privacy of data.
Language Barriers
Language barriers have been identified as another factor that can negatively impact how mHealth technologies can be used, especially in low-resource settings. Although web-based machine language translations continue to improve [39], there is a lack of tailored applications designed to meet the needs of developing counties. For instance, South Africa not only has 11 official languages but many more indigenous ones [40] that are rarely reflected in mHealth technologies. This can cause barriers when using mHealth technologies as it can be difficult to scale up the intervention to address each individual language.
Lack of Training
The education and training of frontline health care workers is also critical when implementing mHealth initiatives in low-resource settings [29]. Chib’s [18] study of midwives in Indonesia showed that although they were comfortable using the basic text messaging and call functions on their mobile phones, they required additional support and training to use more advanced features. The brain drain of highly skilled workers from low-resource settings is another well-documented issue [41] that leaves a shortage of well-educated and technically competent health care professionals to roll out of mHealth programs. Hafkin and Taggart [42] highlight the gender inequalities that exist within developing countries, with women receiving less education than men, leaving them with limited IT knowledge and skills. In the context of developing countries, it is reported that 41% of the population are nonliterate [43], and even the literate among the poor are considered novice users of computer technologies [30]. This directly impacts the implementation of mHealth as many women are health care workers as well as community health care workers.
Poor Technical Infrastructure
The technical infrastructure underpinning any mobile IT system not only consists of mobile devices with appropriate software and operating systems but also reliable mobile networks and protocols for transmitting data [44]. Network connectivity and high bandwidth are important because a slow or regularly interrupted connection can affect the quality of information provided to users. Extant research identifies the reliability and coverage of the network infrastructure as key barriers to mHealth projects [19]. Although mobile phone coverage has skyrocketed in Africa over the last decade [45], it is still not accessible in many rural areas. Unfortunately, the availability of high-speed networks, especially in sub-Saharan Africa, continues to suppress organizations from participating in the economy by using mobile IT [46]. An example of this can be found in the work of Blaschke et al. [47], who reported that a mobile application to monitor childhood nutrition in Malawi was hampered by poor network coverage in some districts. This prevented local community health workers sending SMS messages at the point of care.
Security and Privacy Issues
The implementation of mHealth solutions can also be limited by data security and privacy concerns that arise from legal and ethical issues related to the confidentiality of patient information [48]. These concerns can range from unauthorized access or theft of mobile devices [49], to poor security standards and policies [50], and unregulated or malicious mobile applications [51]. Chang et al. [52] reported mobile devices being stolen during the implementation of an antiretroviral treatment program for HIV/AIDS among peer health workers in Uganda, thus endangering patient confidentiality.
Poor Change Management
Change management is a complex and dynamic process that requires a systematic approach to dealing with change both from the organizational and individual perspective [53]. Effective change management is pertinent throughout implementation, because if this process is poorly managed, it can mean the abandonment of mHealth systems [54]. Wijethilake et al. [55] highlighted that change management in the context of electronic health solutions in developing countries has not been well researched. Mars [56] reports that poor change management can derail mHealth implementation when a tele-rehabilitation system that was rolled out in South Africa failed due in part to poor change management, among other factors.
Potential Barriers to mHealth Acceptance
The next phase of IT implementation in Cooper and Zmud’s model of technological diffusion [12] is acceptance. During this stage, organizational staff are persuaded and encouraged to use the IT application so that it becomes part of organizational work. A review of the literature revealed that this process encounters a number of barriers that can impact the acceptance phase of mobile IT implementation, namely, user resistance, cultural value, practical technology issues, and lack of motivation.
User Resistance
User resistance is defined as “opposition of a user to change associated with a new IS implementation” [57]. Studies indicate that one of the challenges to mHealth remains the acceptability of the technologies to both patients and health care practitioners [19]. Skulimowski [58] posits that clinicians are typically more traditional when it comes to alternatives to face-to-face delivery of medicine. Hasvold and Scholl [59] found that a mobile application, introduced to digitize a whiteboard used to organize patients and surgeries, reduced nurses’ coordination and communication with colleagues. The decreased personal interaction led to strong resistance from nursing staff to and ultimately abandonment of the mobile device as they valued regular professional contact for learning and day-to-day support managing a busy surgical unit.
Cultural Value
Cultural differences that exist in countries may affect behavior in the use and adoption of technology [60]. Culture diversity between developing and developed countries can be observed based on “individualism versus collectivism,” “power distance,” and “masculinity versus femininity” [61,62]. Bofu et al. [63] reports on gender disparity; women and even girls have been sidelined in development issues, and when they attempt to contribute, men have overshadowed them. This highlights, for instance, the cultural values which exist in some developing countries. According to Al Sukkar and Hasan [64], it is unlikely that cultural values can be easily changed or adjusted to conform to any changes introduced by new technology. This conformity, therefore, may have an impact on scanning of organizational opportunities and IT solutions in developing countries. Moreover, Braa and Nermunkh [65] found that because of the contextual constraints, the social system perspective is more critical in the third than in the first world. Any technological solutions that fail to capture local cultural factors in developing countries are often reported to fail [24].
Practical Technology Issues
Practical issues with mobile equipment can hamper the adaptation of mobile IT applications. Commonly cited, practical issues pertaining to mHealth technologies documented in the literature include battery power and screen size [19]. Battery issues are of particular importance in developing countries where electricity supply is unreliable because of insufficient generating capacity and a poor infrastructure [66]. Screen size is another practical issue that can affect the adaptation of mHealth technology. Chae and Kim [67] contend that a small screen combined with increasingly complex functionality can frustrate users of mobile devices. This is due to the fact that users can only view a small amount of information because of the size of the display, forcing them to waste time scrolling repeatedly or performing additional menu selections, which can often lead to navigation errors [68]. Zolfo et al. [69] demonstrate how these problems can be exacerbated in low-resources settings where there is limited access to modern mobile technology. They compared the use of a Nokia N95 to an iPhone among health care workers in Peru and found that the small screen and keyboard of the device limited the physicians’ abilities to access educational material on HIV/AIDS treatment and management.
Lack of Motivation
One of the many challenges when implementing mHealth initiatives in developing countries is adequately motivating the many stakeholders involved at local, regional, and national levels [70]. Farrington et al. [71] cite inertia and the vested interests of different groups, such as health care workers, policy makers, and politicians, for poor progress of mHealth interventions for mental illness in poorer countries. They report this disinterest stems from a desire to maintain the status quo and prevent change, which could potentially revolutionize how the health system operates.
Potential Barriers to mHealth Routinization
Routinization is the second last phase of the Cooper and Zmud [12] model of implementation. At this stage of implementation, the mHealth technology has been utilized in practice for a long period of time, and often cannot be achieved if users face and do not overcome the previously documented barriers. As a result, the use of the technology is not perceived as novel but as a normal activity [72]. From synthesizing the literature pertaining to routinization, one key issue, that is, discontinued use, emerged.
Discontinued Use
Research has shown that the long-term sustainability of any technological solution depends on its continued use as opposed to initial usage [73]. The concept of “continuance” has proven to be instrumental for the success of mHealth initiatives in developing countries as shown by Akter and his colleagues [74,75]. Medhi et al. [31] found that rural health care workers using the CommCare application in India reverted to traditional paper-based data collection methods after a period of time using the mHealth solution. Discontinued use will have a profound negative impact on the implementation of mHealth initiatives in developing countries. That is, the benefits obtained from using mHealth will not translate to the patient and/or clinician, which may not compensate for what is usually a costly and difficult implementation process [16]. In addition, negative perceptions around future mHealth projects may emerge as end users may consider that invested time, effort, and money into a project as wasted.
Potential Barriers to mHealth Infusion
Infusion is the last phase of implementation, where the mobile IT is used to its fullest potential [12]. That implies that the end user utilizes various features that the IT artifact has to offer, integrate the IT in their work, while seeking novel ways of using the IT outside of its intended use [76]. Infusion of mHealth technologies in developing countries is not well documented. The authors therefore examine research surrounding IT infusion and apply it to mHealth. The following barriers have been identified from the literature that can impact the infusion of mobile IT, namely, habit, lack of personal innovativeness, and immaturity of the system.
Habit
The impact of habit on IT infusion has been explored in extant infusion literature [77-78] and found to have a significant effect on infusion. Habit refers to “the extent to which an individual tends to use mobile Health technology automatically (adapted from Limayem and Hirt [79]) often inferred from past experiences” [80]. Limayem and Hirt [82] found that habit plays an important role in explaining usage behavior. Subsequently, Limayem et al. [81] found that habitual routines are often established during the routinization phase, which can hinder infusion of technological solutions [73]. The underlying premise for this argument is that individuals who have made it customary to habitually utilize mHealth technologies in a restrictive manner, become less receptive to novel uses of the technology and, thus, maintain a level of current usage through established ways [78]. Therefore, preestablished methods of performing actions using mHealth solutions may prohibit the user from progressing beyond the routinization phase and not achieving infusion.
Lack of Personal Innovativeness
Another barrier to mHealth infusion pertains to the innovativeness levels of individual users. Personal innovativeness refers to the extent to which a person’s predisposition or attitude reflecting his or her tendency to experiment with mHealth technologies independently of the communicated experience of others (adapted from Schillewaert et al. [82]). That implies individuals must be open to innovate with existing mHealth solutions. As part of their research, Jones et al. [26] found that personal innovativeness was positively related to infusion. The underlying rationale for the strong association between personal innovativeness and infusion is that users who infuse any technological solution are required to use all possible and appropriate applications for both intended and unintended purposes [80]. As a result, a lack of personal innovativeness may restrict the user from experimenting with the mHealth technology and gaining additional insights into how the mHealth technology can be fully applied, thus achieving maximum benefits.
Immaturity of the System
Maturation of technology refers to the degree to which a technology is mature for widespread implementation (adapted from Wu and Subramaniam [83]). Therefore, a technological solution would be considered immature when it has associated system restrictiveness and incompatibility with existing systems. Previous research has demonstrated that mobile IT with a high degree of system restrictiveness had negative impacts on utilization [84,88] as users have no freedom to restructure the system to their own preferences in order to maximize potential benefits. Mobile IT used in developing countries is based on older technologies that offer basic and limited functionality to the end user (i.e., little smartphone use exists). This limited functionality may not facilitate compatibility with existing systems. Nowadays, smartphones offer an array of functionality that integrates previously independent systems (e.g., GPS, camera, and voice/text communication). Yet, there is a paucity of smartphones usage in developing regions. In terms of its immature development status, mHealth in developing regions may not demonstrate the full potentials of mHealth for adopters as the perceived benefits in such regions are not well established. The underlying premise of this argument is that the basic mobile solutions employed by users in developing countries offer specific technological capabilities, which may potentially place constraints on the users.
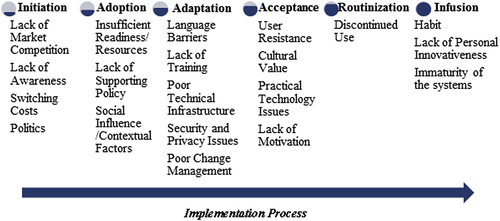
Potential Barriers to Mobile IT Implementation
A summary of the barriers associated with individual implementation phases of the Cooper and Zmud [12] technological diffusion model are presented in Figure 10.2. From the literature analysis, it is evident that phases of the mHealth implementation process experience a collection of barriers or challenges that could have an impact on mHealth implementation. From Figure 10.2, the nature of the barriers provides an insight into the complexity associated with each phase. The following section will discuss this in greater depth.
Discussion and Findings
The findings reveal that numerous barriers could potentially hinder the implementation of mHealth initiatives within developing countries. From reviewing and synthesizing the findings, it is evident that the barriers (a) can be categorized as sociocultural and technological barriers and (b) exist across multiple levels, namely, individual, organizational, and governmental.
The existing state of low-resource countries in terms of the health domain is heavily influenced by their sociocultural traditions. This organizational socioculture is deeply embedded within health processes and is very different to that in developed countries. That is, mHealth initiatives primarily adhere to western designs and fall short of recognizing the unique sociocultural factors associated with developing regions [24]. Sociocultural factors are described by Shier et al. [85] as “those aspects of the social environment that are a direct result of the intersection between the cultural underpinnings of a society (such as a collective system of values, beliefs, and thoughts) and its social processes and organisational mechanisms (such as, social interaction and relationships and institutional dynamics).” Neglecting such sociocultural factors when implementing mHealth could result in failure. When implementing IT (such as mHealth) it is imperative therefore to be aware of the sociocultural aspects involved [86]. Sociocultural barriers to mHealth implementation in developing countries identified in this chapter include lack of market competition, lack of awareness, switching costs, politics (initiation phase); lack of supporting policy, social influence, perceived threat/mismanagement expectations (adoption phase); language barriers, lack of training, poor change management (adaptation phase); user resistance, cultural value, lack of motivation (acceptance phase), and habit (infusion phase).
Addressing sociocultural barriers is only one stepping stone toward resolving issues associated with mHealth implementation in developing countries. Practitioners and academics should be aware of the technological barriers that could hinder the implementation process. Technological barriers are described as limited access to useful, relevant, and appropriate hardware and software, especially in “instances where the use of the technology is perceived as not being sufficient to perform the tasks or accomplish the objectives for which the technology was initially utilised” [87]. Technological barriers are often reported as a significant cause of poor implementation and diffusion rates in developing countries [88]. Technological barriers identified in this chapter that could potentially hinder the implementation of mHealth solutions in developing countries include lack of market competition (initiation phase); insufficient readiness/resources (adoption phase); poor technical infrastructure, security and privacy issues (adaptation phase); practical technology issues (acceptance phase); discontinued use (routinization phase); and immaturity of the system (infusion phase).
Our findings reinforce previous research that the sociocultural, in addition to the technological, dimensions associated with ICT initiatives are essential for successful implementation. Our findings also reveal that barriers to mHealth implementation exist across various stakeholders at different levels within the health system. That is, barriers to mHealth initiatives are observed at the individual, organizational, and national level. The majority of the barriers are identified at the organizational level. Despite this, all levels identified are interconnected and require effective communication and collaboration to facilitate the successful implementation of mHealth initiatives. At the national level, appropriate policies, procedures, and ethical and legal frameworks should be established to ensure that organizations and, subsequently, can implement mHealth initiatives. This finding argues that implementing mHealth initiatives requires multistakeholder input.
Conclusion
One approach to ensuring that mHealth initiatives can be successfully implemented and used is to identify barriers to implementation. For developing countries, to date a vast array of research exists that focuses on barriers to generic IT adoption; however, the majority of these papers embrace the concept of adoption to cover the entire process of implementation. As outlined earlier, implementation of IT artifacts occur over six phases (Table 10.1). This chapter makes a very clear contribution to both theory and practice. The barriers for mHealth deployment within a developing country setting are presented under each of the six implementation phases. This provides a high degree of granularity, which in turn enables the authors to classify the barriers from a sociocultural and technological barrier perspective. This degree of detail will greatly increase the chances for success when mHealth solutions are deployed within low-resource settings.
To our knowledge, Cooper and Zmud’s model has not been utilized in this manner in other studies of mHealth in low-resource settings. Although this chapter has sought to identify barriers that occur at each phase of mHealth implementation, our approach has some limitations. First, the exploratory nature of the literature has meant that a rigorous or systematic search of the literature was not undertaken. This could result in the omission of additional barriers to mHealth implementation in extant literature that has not been included in our results. In addition, most case studies that were used did not explicitly state the phase of implementation being undertaken, so our interpretations were based on evaluating Cooper and Zmud’s definitions against the description of the mHealth initiatives uncovered in the literature. Although every effort was made to identify the correct phase of implementation in line with the Cooper and Zmud model, the barriers outlined above are based on our interpretation and we would actively encourage future research in this area to describe in detail how mHealth programs are implemented. That being said, the taxonomy of barriers to mHealth implementation presented in this chapter underpins the key issues that occur when rolling out an mHealth program in a developing country.
This chapter provides for the first time a detailed step-by-step breakdown of the implementation process for mHealth in developing countries. Future research should focus on a qualitative systematic review to take into account the complex nature of mHealth implementations to provide a higher degree of rigor in the research findings. This will help to ensure that mHealth solutions will have a greater chance of success when implemented within low-resource settings.
..................Content has been hidden....................
You can't read the all page of ebook, please click here login for view all page.