
Chapter 13
Telehealth in Primary Health Care
Analysis of Liverpool NHS Experience
Nonso Nnamoko1, Farath Arshad1, Lisa Hammond2, Sam Mcpartland3, and Pat Patterson2 1Centre for Health and Social Care Informatics – CHaSCI, Liverpool John Moores University, Liverpool, UK 2NHS Liverpool Community Health, Wavertree Technology Park, Liverpool, UK 3Primary Care Commissioning IM&T Team, Informatics Merseyside, Liverpool, UK
E-mail: [email protected], [email protected], [email protected], [email protected], [email protected]
E-mail: [email protected], [email protected], [email protected], [email protected], [email protected]
Abstract
This chapter describes a feasibility study that examined user experience of a telehealth system within a local area in the United Kingdom. The telehealth system was designed by Philips (called Motiva) and piloted within Liverpool National Health Service (NHS) Primary Care Trust (PCT), United Kingdom. The telehealth system operates a dual interface and real-time data transfer mechanism that allows patients to upload and monitor vital signs (e.g., weight and blood pressure) from their own homes, which are comonitored by clinicians to provide adequate intervention. The pilot project spanned a period of 6 months, and a questionnaire/interview study was conducted among the two user groups (i.e., patients and clinicians); prior to this, a pilot study was used to uncover their experiences. Questionnaire responses were recorded from 24 patients with various Long Term Conditions (LTC), and four of them were followed up for a one-to-one interview. Questionnaire and interview responses were recorded from 12 clinicians (including 7 Matrons, 3 Nurses and 2 GPs). The data analysis showed: 87.5% of patients were satisfied with the telehealth system; 87.50% received more support at home; 91.67% understood and managed their condition better, and 95.83% felt re-assured knowing that their readings were comonitored by clinicians. There are proven indications that hospital/general practitioner visits were reduced as a result. Clinicians’ results were also positive, with 85.71% expressing their satisfaction with the pilot system and telehealth technology in general. Telehealth holds great promises for improving clinical management and health care services delivery by enhancing access, quality, efficiency, and cost-effectiveness.
Keywords
National Health Service (NHS); Telehealth; Patient Experience; Vital Signs; Clinical Management; Community MatronsIntroduction
Increasing health care cost and managing patient expectations has called for a rethink in the way health care is provided in the United Kingdom. Current service transformations are relying significantly on harnessing the advantages that may be possible through greater use of the information and communication technology (ICT) infrastructure already in place within the UK National Health Service (NHS). Certainly, the drive to deliver out-of-hospital care, which promotes immediate and tailored support to patients in a cost-effective manner, is receiving much attention, especially now that health service providers struggle to cope with the rising numbers of elderly people, particularly those with long-term conditions (LTCs) [1]. Telehealth is receiving increasing interest within the NHS as a means to deliver health care from a distance. This is partly because improvements in technology is making the medium faster, cheaper, and easy to use, but even more encouraging has been its use to engage with hard-to-reach groups [2]. This effort to move services closer to patients is believed to help the NHS achieve good-quality health care delivery, at a time and place suitable to patients while remaining within the financial envelope. However, with interest on telehealth technologies now widespread, academics fear that local health communities are being left without the information they need to effectively roll out the technology [3]. Whereas the impact of telehealth technologies in health care has received huge coverage, the area of user experience is still underresearched [4].
This chapter describes and analyzes the process of incorporating a telehealth system (Motiva) on a 6-month pilot project within the Liverpool local NHS, United Kingdom. The Motiva system was developed by Philips, and offers remote management facility to patients with LTC [5]. The implementation relied on clinicians who otherwise operate a conventional care delivery method that is more hospital based. The Centre for Health and Social Care Informatics (CHaSCI) at Liverpool John Moores University (LJMU) conducted a feasibility study after the pilot. The study reflects the aim of the pilot, which sought to strengthen the quality of primary care delivered to patients and also to educate clinicians on the use of telehealth systems. In addition, the study provides detailed insight into user experience of the telehealth system. For both patients (including carers) and clinicians involved in the pilot project, a quantitative and qualitative exercise was carried out through paper-based questionnaire and one-to-one semistructured interviews, respectively. The sources for this analysis include information from related research and documents from the funding institutions that worked closely with both Philips and CHaSCI to structure and deliver the overall project. The study procedure and key findings forms the core of this chapter but first, we describe the components of the telehealth project. The Conclusion and Recommendation sections highlight areas that may be influential in deciding on the direction of travel for the telehealth work stream within the local health economy.
Characteristics of the Motiva Pilot Project
In 2010, Liverpool Primary Care Trust (PCT) was approached by Philips with the opportunity to run a proof of concept using assistive telehealth in the local area for a limited time period. The key objectives were to evaluate the use of assistive telehealth technology to
• identify if the perceived benefits in the use of telehealth technology can be demonstrated, including associated cost savings and patient experience;
• evaluate how telehealth can support the clinical pathways developed as part of the Quality, Innovation, Productivity and Prevention (QIPP) agenda [6];
• identify key lessons learnt from the proof of concept that can support and facilitate any future rollout of telehealth locally, including the identification of any dis-benefits associated with assisted telehealth; and
• identify opportunities to change the way that local health care is delivered to patients suffering with long-term conditions.
The motivation for this study came from Liverpool PCT’s need to understand patients’ perception of the system, the impact of the system on patient welfare, and on clinician workload. In addition, because an earlier preliminary study (with five patients) was not successful, Liverpool PCT and the system manufacturer (Philips) both wanted an up-to-date report of the system usage to assess if there is need for further modification(s).
Cohort Recruitment and Time Scales
The proof of concept pilot was undertaken in three phases, each spanning a period of 3 months. Phase 1 was conducted with patients diagnosed with heart failure (HF) only. Phase 1 did not work as anticipated because the daily monitoring was done by lower-qualified clinical staff and there were issues regarding the cohort (i.e., involved HF patients only from one health center). Therefore phase 1b was considered with a different approach; recruiting patients with chronic obstructive pulmonary disease (COPD) and diabetes in addition to those with HF. Patients were also recruited from other health care providers managed by Liverpool Community Health in the Anfield area of Liverpool. This time, the telehealth monitoring exercise was undertaken by highly qualified clinical staff (community matrons). This model was successful and enabled the phase 2 pilot in which patient recruitment was extended to another team of community matrons based in the Edge Hill area of Liverpool. New patients were recruited during phase 2 but patients enrolled onto phase 1b were kept on the system as part of phase 2.
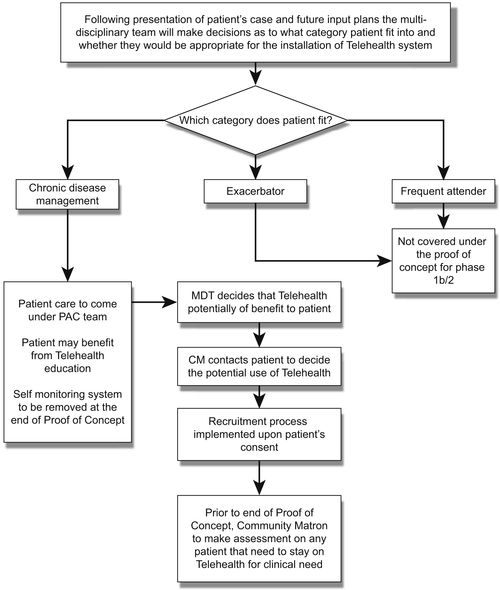
The recruiting community matron(s) were responsible for obtaining patient consent and ensuring that the patients’ general practitioners (GPs) were informed. The community matrons at Everton Road Health Centre monitored the patients on a daily basis (Monday–Friday) during phase 1b. For phase 2, the matrons at Edge Hill Health Centre were also involved in the monitoring process. Figure 13.1 shows the selection method used to identify patients potentially suitable for inclusion in the pilot study. The analysis reported in this chapter was deemed to be of an audit nature, and so ethical approval was not considered necessary by the NHS provider.
Once patients commenced on the telehealth program, they began to send their vital signs for review. Patient data was recorded automatically using compatible monitoring devices supplied with the system (Figure 13.2) and transmitted to the system’s back end. Patients must complete the monitoring exercise every day of the week (Monday–Sunday) before 11:00 AM. Generally patients recorded their blood pressure and weight as a standard. In addition, diabetic patients would record their blood glucose levels whereas patients with COPD would record their saturation levels. Clinicians must access and review captured data after 11:00 AM each working day (Monday–Friday).
The matrons would use their own clinical judgement to assess the patient’s results on a daily basis and treat accordingly. Patients also received educational videos on the chronic disease area they were being monitored for on the telehealth program. The analysis and results provided in this chapter covers phases 1b and 2 only and provides answers to the objectives outlined in the previous section.
Method
The study was conducted among two user groups (i.e., patients and clinicians) using two survey approaches—a simple questionnaire focused on the system use, followed by a second more general one-to-one discussion about telehealth and its impact on user roles/duties. The questionnaire consists of a range of multiple-choice questions about user experience/satisfaction of the telehealth system, and spaces for free text comments.
An earlier test study had been conducted by Philips, and some of their questions were adapted and incorporated into the version reported here. (Note: Philips had only tested the system with five patients, and the NHS provider required an objective view of the patient experience with the proof of concept telehealth work, hence the commissioning of the study undertaken and reported in this chapter.) Key lines of inquiry are shown in Tables 13.1 and 13.2.
Paper-based questionnaires were distributed to patients (n = 45; 24 of 45 = 53% response rate) who took part in the system pilot, along with a self-addressed stamped envelope to receive replies. Nonresponders were not followed up because of time limitations. All 24 respondents had already completed the clinical trial when they answered the questionnaire, although some used the system more than others because of a series of changes made during the pilot as detailed in the previous section. A follow-on interview was arranged with a small sample of patients, selected based on mobility (n = 6; 4 of 6 = 67% response rate). Patient attrition rate was attributed to three factors: despondency, delay in return (note: we had limited time scale to undertake the study and produce a report), and withdrawal from scheduled appointments. The clinician survey took a similar approach, complementing targeted questionnaire study with semistructured interviews. However, both study phases for clinicians were conducted consecutively per subject so they were first asked to complete a prevalidated questionnaire, followed by a semistructured interview. In total, 12 clinicians including 7 matrons, 3 nurses, and 2 GPs were considered. However, as only the matrons and nurses had direct involvement with the telehealth system, we conducted the full study (questionnaire and interview) with them, and approached the GPs for general opinions on telehealth. The nurses’ opinions were sampled via telephone as face-to-face interviews could not be arranged in time.

In view of the heterogeneous nature of the questionnaire content and its administration method (paper-based), the data available did not permit the use of formal statistical techniques for analysis. Instead, we report a broad qualitative and quantitative analysis of the findings (similar to narrative synthesis). Although several published methodologies exist for analyzing heterogeneous data [7,8], they are often domain or subject specific, time consuming and mostly used in large-scale analysis. The method used in this chapter is suitable for analyzing studies with diverse outcomes [9] and indeed a standard practice within the health care domain for analyzing heterogeneous data sets [10,11]. We gauged patient experience using their individual and collective responses to the questions. We did not use a formal scoring method as no well-validated generic instrument for automatic review of such a questionnaire with diverse content exists yet for end users [9].
Table 13.1
Key Lines of Inquiry Covered in the Quantitative (Paper) Study
| Section No. | Patients’ Questionnaire | Clinicians’ Questionnaire |
| Section 1 | First impressions about Motiva (4 embedded questions) | First impressions about Motiva (4 embedded questions) |
| Section 2 | Effects of Motiva on care pathway (12 embedded questions) | User satisfaction/performance (4 embedded questions) |
| Section 3 | User perception (15 embedded questions) |
Table 13.2
Key Lines of Inquiry Covered in the Qualitative (Oral) Study
| Question | Semistructured Interview with Patient(s) |
| 1. 2. 3. 4. | Highlight the most negative/positive aspect(s) of the Motiva system from your point of view Did you learn anything new from the process? Is there anything else about being involved in the telehealth project that you wish had been different? Is there anything else you think we have not covered on the questionnaire with regards to your experience? |
| Semistructured interview with clinician(s) | |
| 1. 2. 3. 4. 5. | Highlight the most positive/negative aspects of the project? Did you learn anything new about telehealth technology in general? How has the use of telehealth affected the tasks you would normally undertake? That is, has the load increased or decreased? Do you feel more confident about new technology now? Is there anything else about being involved in the project you wish had been different—including those not covered in the questionnaire? |
Analysis and Result
Patients
As background, 24 and 4 patients were considered for the quantitative (questionnaire) and qualitative (interview) studies respectively. We first asked users to indicate the condition for which they were enrolled on the pilot project, before completing the different sections of the questionnaire (see Table 13.1). Of the 24 respondents, 18 were identified as having COPD, 5 were HF patients, and only 2 have diabetes.
Questionnaire Section 1: First Impressions (Embedded Questions 1–4)
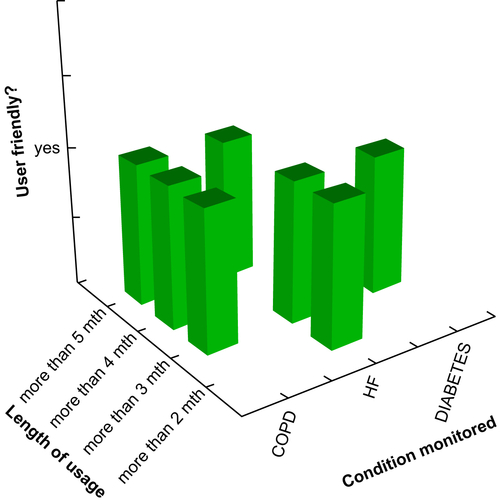
All respondents (100%) indicated they received adequate information/instructions about the pilot (telehealth proof of concept) project and the system usage prior to installation. We also asked users to rate their first experience using the system with five options (i.e., outstanding, satisfactory, neutral, poor, or very poor). There was strong indication from the response that their experience was average at the least. Majority (54%) said it was outstanding, 37.5% said it was satisfactory, and the remaining (n = 2) answered “neutral.” When asked if the system was user friendly and how long they had used it, all 24 patients, regardless of length of usage, indicated that the system was easy to use. Majority (92%) used the system for at least 3 months, and the other 2 patients used it for a little under 3 months (Figure 13.3). This result is very important as it eliminates bias in subsequent findings.
Questionnaire Section 2: Effects of Motiva on Care Pathway (Embedded Questions 5–16)
To gauge the impact on care pathway, we asked users 12 questions (mostly yes or no type) with space for further comments (optional). For simplicity, we arranged user responses to the yes or no type questions (n = 6) into Table 13.3. The other 6 questions are explained in a question/response format.
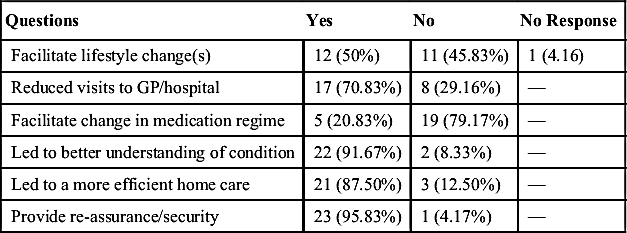
In line with recent findings on telehealth outcomes [12], the monitoring of vital signs via the telehealth system reassured patients (95.83%), empowered patients (91.67%), improved care at home (87.50%), and reduced hospital/GP visits (70.83). Additional comments supplied by respondents suggest that patients and their family felt reassured knowing that monitoring and help were available. Also, the cumulative trend visualization of measured signs along with other on-screen help led to better understanding of the condition. Most respondents who experienced improved home care stated that communication with clinical staff was improved, discussions were tailored, and visits (GP or hospital) were only arranged when necessary. Basically, patients monitored from their own homes, received help from clinicians at any occurrence of abnormality in measurements observed. This is important as research suggests that older patients prefer care at home through self-management rather than institutional [13]. However, care must be taken to ensure adequate contact is maintained because some patients, particularly the elderly who often live alone, value the social contact with clinicians [14]. Some researchers argue that home care through telehealth reduces close contact [15,16], and data/information integrity may be undermined [2], resulting in poor clinical decisions and distrust between patients and clinicians. In contrast, this project enhanced the clinical care and immediacy of response to accommodate patient needs, perhaps because of the implementation strategy and/or the organizational structure of the local NHS provider.
Table 13.3
System Effects of Motiva on Patients’ Care Pathway
| Questions | Yes | No | No Response |
| Facilitate lifestyle change(s) | 12 (50%) | 11 (45.83%) | 1 (4.16) |
| Reduced visits to GP/hospital | 17 (70.83%) | 8 (29.16%) | — |
| Facilitate change in medication regime | 5 (20.83%) | 19 (79.17%) | — |
| Led to better understanding of condition | 22 (91.67%) | 2 (8.33%) | — |
| Led to a more efficient home care | 21 (87.50%) | 3 (12.50%) | — |
| Provide re-assurance/security | 23 (95.83%) | 1 (4.17%) | — |
The community matron’s role was introduced into the United Kingdom in 2005 in order to reduce unplanned hospital admissions of patients living with long-term conditions, and their services largely involves visits to patients’ homes [17]. This service level was maintained during the pilot period, and consequently GP/hospital visits were reported to have reduced. This result shows a positive effect of the matrons’ job role and echoes research findings that telehealth reduces hospital visits [18] and associated cost [2], by enabling individuals to perform certain tasks at home. Most respondents who reduced the number of visits to their GP wrote that complications were detected early and dealt with promptly via telephone discussion(s) and/or in some cases, a matron visiting them at home. In addition, some of those who did not reduce GP/hospital visits revealed that this was in fact a positive outcome. One respondent was placed under intensive care because the system revealed some potentially dangerous fluctuations in their measurement. Another wrote that visits remained the same because they “had to attend regardless.”
Half of the respondents agreed to have made lifestyle changes particularly in improving exercise regime and diet control. The other half (less one patient who did not respond) did not make lifestyle changes, but additional comments suggest their response had more to do with their health and/or physical status levels. For instance, one respondent wrote “No reason to”; others wrote “breathing problems,” “difficulty walking, painful legs,” “I find it difficult to get weighed without the scales supplied with the system.” We also noticed that majority (79.17%) had not made changes to their medication regime as a result of using the system. Examination of the additional comments indicates they had no need to make changes. Of those who did (20.83%), some added it was in response to rapid changes in measurements observed through trend visualizations. Basically, some patients had all or part of their medication(s) altered to reflect changes in their measurements, and others became more aware of therapeutic solutions to changes in their measurements. For instance, one respondent wrote, “Just better understanding of when to use medicines”; a comment among others which echoes that the system led to better understanding of condition according to results (see Table 13.3).
In other questions (not shown in Table 13.3), we asked users to identify in one of three options (increased, the same, reduced) their observations regarding clinical support since the introduction of Motiva. (Recall: study was conducted after the project, so this includes the period after the pilot.) Of the 23 patients who responded to this question, 30.43% (n = 7) said support increased and 65.22% (n = 15) said it stayed the same; another indication that the local NHS organizational setup played a part in the success of the pilot as explained earlier. The only respondent who experienced reduced clinical support added, “Have not needed to see my Matron as much.” In addition to on-screen visualizations of measurement trends, the system provided patients with educational videos to explain their condition, so we asked respondents if they watched the regular educational video clips presented daily through the system. Those who answered “Yes” had five other related questions to complete (Table 13.4) and those who answered “No” were asked to explain why before they continue with the last section of the questionnaire.
Overall, 16.67% (n = 4) of the respondents neither watched the videos nor provided comments to explain why. However, the rest (n = 20) watched the videos and attempted all or part of the follow-on questions.
Questionnaire Section 3: User Perception (Embedded Questions 17–31)
Respondents were asked to rate their perception of Motiva services toward better understanding of their condition. As expected, the majority of respondents were either extremely satisfied (n = 13) or very satisfied (n = 8). The remaining 3 were not sure (neutral). Respondents were also asked specific questions about elements of the system they liked or disliked (Table 13.5), and other questions regarding their experience with the system and telehealth in general (Table 13.6).
Almost two-thirds of the respondents (62.5%) liked the educational information supplied, and the rest did not answer the question. As expected, a large percentage of respondents liked the fact that their measurements were being tracked (95.83%) and help was always available (78.26%). Majority (95.83) also liked monitoring regularly but unsurprisingly a high percentage (79.16%) felt it was regimented (i.e., on or before 11:00 AM each day). Because the matrons owe the same duty of care, which largely involves visits to patients’ homes [17], and the conventional method has been proven to improve patient’s quality of life [19][20], the set time for telehealth monitoring exercise is inevitable. This means that patients’ measurements must be transmitted in time for clinicians (matrons and nurses), who have to review them and still carry out other duties such as home visits as required.
Table 13.4
Abstract of User Responses to the Relevance of Educational Videos
| Q | Was enough effort made to encourage you? (20 responded) |
| A | They all agreed that enough effort was made. |
| Q | What encouraged you? (13 responded) |
| A | Most respondents agreed that the videos came-up automatically and were easy to follow. One patient added, “….understanding my condition and how I could try to ease my breathing.” Another wrote, “felt less isolated knowing other people unfortunately have similar problems.” |
| Q | What did you find most useful about the videos? (15 responded) |
| A | Most respondents agreed they were informative, providing clear explanation of their condition. Some wrote that the videos helped them make lifestyle changes. |
| Q | What was not so useful about the videos? (7 responded) |
| A | Of the 7 respondents, 6 found everything useful, with one adding, “Was on a course so I knew some of the information.” However, one respondent found the videos frightening, adding that “it revealed the dangers associated with bad management.” |
| Q | What additional videos would you like in the future? (7 responded) |
| A | Respondents were mostly satisfied with available videos but one of them added that they would like to see statistics showing how they compared to others with similar condition, in terms of management. |
Table 13.5
Patients’ View of Liked and Disliked Elements of Motiva (Quantitative)
| Questions | Like | Dislike | No Response |
| Educational information to manage condition better | 15 | — | 9 |
| Knowing measurements are being tracked | 23 | — | 1 |
| Knowing I can always contact clinicians if I have concerns | 18 | — | 6 |
| Having to monitor regularly | 23 | — | 1 |
| Having to monitor within set times (regimented) | 19 | 4 | 1 |
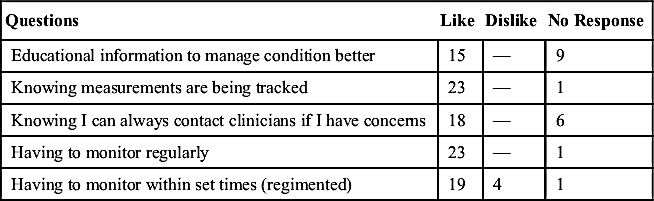
Table 13.6
Patients’ Experience/Perception of Motiva and Telehealth in General
| Questions | Yes | No | No Response |
| Would you like telehealth in other aspects of your health | 16 | 8 | — |
| Did you experience any kind of system failure with Motiva | 12 | 12 | — |
| Would you recommend Motiva | 23 | — | 1 |
| Would you consider telehealth in the future | 21 | 2 | 1 |
| Would you like to continue using Motiva | 20 | 3 | 1 |
| Would you like to see changes to enhance Motiva service(s) | 4 | 19 | 1 |
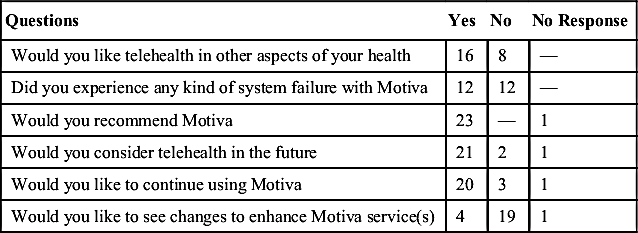
As expected, majority of the respondents (66.66%) would like telehealth in other aspects of health care. Overall, 83.33% want to carry on using the system, 95.83% would recommend it, and 87.5% would consider telehealth in the future. Half of the respondents experienced system failure, and a small percentage (16.66%) would like to see some changes made to the system. We also asked what follow-on support they would like to see after the pilot, and only 50% responded. Among their suggestions were regular contact and/or educational health care information via phone (50%), e-mail (25%), or post (12.5%). One respondent added they would like a dedicated discussion forum guided by experienced clinical staff members. We observed that this section of the questionnaire was sparsely completed, and there was little evidence to explain the responses supplied, perhaps because of the survey length. According to Frede [21], the longer the survey, “the fewer respondents complete it and the more drop out.” We knew this could adversely affect quality, so we included some of the questions (with low response rate) in the semistructured interview to obtain more information.
Semistructured Interview (Four Embedded Questions)
Because all 24 respondents agreed the system was user friendly regardless of the length of usage and/or condition monitored (Figure 13.3), we focused on functionality of the system and impact on patient health, especially areas of the questionnaire that lacked evidence (additional comment) or those with low response count. We asked if they learnt anything new about their condition through the period they used the system. All 4 respondents agreed they had learnt one or more facts about their condition, particularly around “breathing technique.” We then asked them to highlight the most negative/positive aspect(s) of the system from their experience (Table 13.7). The most disliked element centered on the frequency of measurements required. Of the respondents, 3 (of 4) reported that the frequency at which some of the variables (e.g., weight and blood pressure) were requested was inappropriate. For instance, one respondent said that daily prompts to measure weight for a well-managed diabetes case would be unnecessary, hence the need for a personalization option within the system. Another added that “blood pressure varies at different times of the day but the test was only conducted once daily.” The intention was to use Motiva to drive service improvement that would see patient self-management and education as an integral part of the care offered; resulting in longer-term goals of reducing hospital outpatient referrals and admissions.
Table 13.7
Patients’ View of Positive and Negative Aspects of Motiva (Qualitative)
| Positive(s) | Negative(s) |
| Ability to visualize and track measurements Easy to use Boosts confidence Reassured knowing that measurements are being tracked by clinicians Educative and effected lifestyle changes | Frequency of measurement, especially weight. System failure/Internet connectivity issues |
As expected, many users experienced system failure at some point during the process but explained that these were often minor technical issues and were promptly managed by the technical support team. Despite the negatives highlighted, patient satisfaction with the system was high. All respondents (n = 4) expressed their dissatisfaction with the project ending. This result was captured when we asked respondents to highlight anything they wish had been different about the pilot system, including items not covered within the questionnaire. One respondent added that “confidence level has dropped since the termination.” Further comments suggest they would in fact like to see something else put in place after the termination, particularly to help maintain the same level of communication with clinicians.
Clinicians
This cohort comprised 12 clinicians, made up of 7 matrons, 3 nurses and 2 GPs. The feasibility study was conducted in two parts eliciting quantitative (Table 13.1) and qualitative (Table 13.2) data. GPs were only approached to sample their opinions on telehealth, as they had no direct contact with Motiva. The results reported in the questionnaire section consists of 10 clinicians only (i.e., excluding GPs). We included GPs’ opinions within the semistructured interview section.
Questionnaire Section 1: First Impressions (Four Embedded Questions)
Majority of the clinicians (80%) used the system at least 3 months before the pilot ended. The other 20% used it a little over 2 months. We asked if users were provided with adequate information and training prior to use with three options (yes, no, not sure). Majority (80%) answered “yes,” and the rest (20%) were not sure. One respondent who was not sure added, “Training was brief and I have poor computer background,” suggesting this could be due to poor computer literacy, and some clinicians are less receptive to the use of new technologies [22]. We then asked users to rate their first experience using the system with five options (i.e., outstanding, satisfactory, neutral, poor, very poor). Majority (70%) had either an outstanding (n = 2) or satisfactory (n = 5) experience. Those who had either poor (n = 2) or very poor (n = 1) experience agreed (in additional comment) that they struggled at the beginning because the system was imposed on them and they have poor computer background. One added, “it was time consuming and took a huge amount of time out of daily schedules.” Unsurprisingly, two of the three users who had either poor or very poor first experience answered “no” when we asked if the system was user friendly. However, majority (80%) found it easy to use.
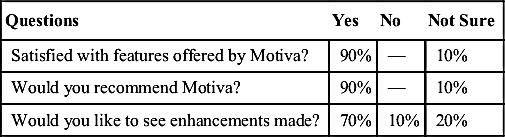
Questionnaire Section 2: Performance and Satisfaction (Four Embedded Questions)
We asked users to rate their satisfaction level with Motiva services in understanding their patients. Five options were provided (i.e., extremely satisfied, very satisfied, neutral, very dissatisfied or extremely dissatisfied). Only eight users responded to this question, of which three were neutral, four were very satisfied, and one was extremely satisfied. We were unable to establish the reasons behind their choices because there were no additional comments to explain these choices even though we had included related questions in the semistructured interview as detailed in the following section. Other questions revealed that the system was fit for purpose but could benefit from further modifications (Table 13.8). Majority (90%) were satisfied with available features and would in fact recommend Motiva, although a good number of users (70%) would like to see some changes to further enhance the system.
Semistructured Interview (Five Embedded Questions)
To establish the underlying reasons behind some of the user responses in the questionnaire, we asked respondents to highlight the most positive/negative aspects of the project and to explain how telehealth affected the tasks they would normally undertake. (i.e., has the load increased or decreased?). We discuss their responses to both questions in parallel and explain results of other queries posed.
Respondents were particularly happy with Motiva services in facilitating quick assessment and timely intervention. In fact, all respondents agreed they responded quickly to patients during the pilot, solely based on the wealth of patient information received on a daily basis. Respondents added that patients had expressed to them feeling safer, independent, and understood their condition better (70%); interventions were tailored to patient needs (80%), and they reported that unnecessary hospital visits were reduced as a result (100%). In contrast to suggestions that home care through telehealth reduces contact with clinicians [9], the study results show that home visits to patients either increased (70%) or stayed the same (30%) during the pilot. The matrons attributed this to organizational setup and the Motiva operational model. Prior to the pilot project, matrons had a caseload of patients with whom they agreed individualized care plans, along with GPs and other staff. The plans, along with agreed patient’s data sets, are then shared in confidence among clinicians through a central system called EMIS Web [23]. The Motiva clinical interface however generalized the client (patient) base by displaying the entire cohort, with masked patient biodata and risk alerts sorted by priority. Remote monitoring has been shown to be an efficient use of resources [2], [18] because clinicians were able to monitor and analyze the data at the office, thereby freeing time for conducting other examinations or for seeing more patients. However, clinicians were forced to monitor any patient, with or without prior knowledge of their health status, which resulted in other issues as follows.
Integration
Majority (90%) agreed that lack of integration with the current system (EMIS Web) caused delay in intervention. When faced with unfamiliar patients, clinicians would refer to EMIS Web for assessment before intervening. Majority (90%) agreed there was increased time loss because of this unfamiliarity. One respondent said, “I spent huge amount of time each day reading unfamiliar patients’ history.”
Flexibility
The system was designed to run a full 7-day week rather than the 5-day week arrangement within the participating NHS service provider, so clinicians experienced huge time loss on Mondays in dealing with backlogs. That is, measuring data captured over the weekend was accessed on Mondays. In addition, users highlighted that default the setting of the system does not allow for personalized care. For instance, baseline (upper and lower limits) and monitoring frequency of variables (e.g., weight) are rigid and could not be tailored to patients’ individual needs. One respondent added that “some patients do not need to monitor their weight daily.” Others said “the default settings automatically override any changes made,” “I often rang patients who did not require attention because the system raised false alarm,” “safe blood pressure limits differ among individuals,” etc. There were also concerns regarding the set monitoring time (on or before 11:00 AM each day), as a small percentage (30%) found it regimented. The system raised a false alarm whenever a patient failed to monitor within the cut-off period each day.
Speed
Respondents experienced low transfer speed at times perhaps because of firewall setting and general web traffic issues. Majority explained (70%) that this happened around the same time each day, thus reducing time for field work (i.e., home visits).
Other areas that raised some concern were centered on the appropriateness of the patient cohort. The majority (60%) agreed that some of the patients did not need telehealth, and a majority of those who would benefit from it were left out of the pilot. Some (50%) said the system was imposed on them and hence they struggled at the beginning. A small percentage (20%) argued that the system caused anxiety among patients. Despite the negatives, majority (80%) said they learnt new things about telehealth and almost two-thirds feel more confident now about new technology. When asked if there are other things about being involved in the project they wished had been different, including those not covered in the questionnaire, most of them echoed some of the negative aspects outlined above. There was also a debate about who should be in charge of the system. Half the respondents (50%) said it is a waste of expertise asking highly qualified staff (matrons and nurses) to be in charge, 20% said some part should be handled by junior staff members (i.e., health care assistants [HCAs]), 10% believed it should be completely handled by HCAs, and the rest were indifferent.
The one-to-one interviews with the GPs showed support for benefits telehealth can bring for patients by focusing on remotely reviewing trend data to decide on follow on action, i.e. arrange visits or appointments with GPs or hospitals without patient/carers explicitly having to do so. There was recognition that such technology will enable patients to remain independent and safe allowing prioritizing of patient needs much more effectively. The two GPs interviewed did both point out that such technological interventions as telehealth needs careful planning, resourcing and training.
Limitations
The sample size reported in this study was small due to a number of reasons. As with similar pilot projects [24], only a small number of patients (n = 45) were enrolled. Although all patients had the opportunity to provide feedback on their experience, only 24 took the opportunity. We were unable to follow-up nonresponders because of time constraints. Also, more input from other GPs within the locality would have been useful to back up the general support identified.
Conclusion and Recommendations
Our findings show overwhelming support for the telehealth project from both user groups. Telehealth holds great promises for improving clinical management and health care services delivery by enhancing access, quality, efficiency, and cost-effectiveness [25,26]. In particular, telehealth can help reach out to patients generally underserved traditionally because of the nature of their illness or age, for example, those with LTC who require constant monitoring and the elderly, especially those technically incapable of moving [25]. Further, evidence points to important socioeconomic benefits to patients, carers, clinicians, and the health care providers, including educational opportunities and enhancements to patient–clinician communication [27]. In order of number of responses and comments received, some of the strongest outcomes of this study were centered on reassurance, education, effective home care, and reduced GP/hospital visits. Our result shows that patients felt reassured, and this was echoed by clinicians during their interview sessions. The ability to take specific measures every day and to see the results fostered a sense of well-being for patients. This also applied to those patients who sometimes forgot to take their readings—leading to the clinician calling to check that all was well. Patients also became more knowledgeable about their illness. In contrast to some research findings [15], we observed some improvements in communication (physical or via telephone) between patients and clinicians. GP/hospital visits were also reduced.
Clinicians considered in this study have wholeheartedly supported telehealth, commending its many features to enable patients to remain independent and safe. This according to most clinicians is largely due to the security offered through real-time monitoring at a distance and scheduling tailored follow-on care quickly. Particularly, it was recognized that telehealth technology brings huge advantages in terms of the speed with which decisions could be made, and extension beyond the pilot period would be considered of benefit. Clinicians reported of patients’ disappointment at the telehealth pilot coming to an end, and this was echoed by patients themselves during the one-to-one interview session. Although support for telehealth is strong, it would have been useful to have conducted the feasibility study over a longer period. More patient feedback would have been captured if time had been allocated to follow up on patients who had not returned their questionnaires. Studies of this nature needs adequate time and scheduling within the overall program of work.
Acknowledgments
Funders: Liverpool Community Health (LCH); Informatics Merseyside (IM); Liverpool Primary Care Trust and Philips (especially for the discussion and images provided by S. Douglas). Our thanks also go to all the matrons, GPs, and patients who gave up time to provide valuable input for the study.
..................Content has been hidden....................
You can't read the all page of ebook, please click here login for view all page.