Chapter 3. Applicability of Six Sigma in Healthcare Organizations
Sections
A Brief Explanation of Six Sigma
Six Sigma Applied to Healthcare
Six Sigma at Work in Healthcare
Different Views of Healthcare Quality
We hope by now we have presented you with enough information about healthcare systems around the world that you will agree that they need to be reformed. We need to start measuring our healthcare failures in deaths per million, not deaths per “hundreds or even deaths per thousands.” Even deaths per million is not good enough in the healthcare system. The required standard should be measured in the deaths per billion and errors per million. This is where proven, preventative approaches—such as Total Improvement Management, Six Sigma, and Lean—can provide real benefit to the healthcare system. Both of these two approaches have been refined as they were used in other industries, and they are now ready to advance the healthcare industry into a new, higher level of customer satisfaction and performance.
Studies indicate that the services industries have an average sigma level of between 2.0 to 2.5; that’s an error rate of 159,000 to 208,000 per million opportunities. But many of the healthcare activities perform much worse. For example, the process for treating depression is estimated to be running at the 2 sigma level or 308,538 errors per million opportunities.
Although process capability techniques have been used extensively in manufacturing for more than 50 years, a major breakthrough occurred when Motorola applied them to its business support functions as a logical extension of its manufacturing quality initiatives. The results were improvements of ten times to a hundred times in Motorola’s business processes in as short a period as two years. When Motorola won the Malcolm Baldrige Award in 1988, it credited the Six Sigma program as the primary driver of its improvement. During the first part of the 1990s, the Six Sigma program continued in Motorola and spread slowly into other organizations. But in the mid-1990s, GE latched onto the concepts and committed millions of dollars to implementing the program throughout the entire organization. GE’s program expanded from 200 projects in 1995 to 6,000 projects in 1997, which resulted in more than $320 million in savings, all directly attributed to this Six Sigma program. In 1998, GE estimated that its savings were about $750 million.
Notable healthcare Six Sigma projects include North Shore-Long Island Jewish Health System, Memorial Hospital and Health, of Marlton NJ, McLeod Regional Medical Center, Froedtert Memorial, New York Presbyterian, Vytra Health Plans, several Blue Cross and Blue Shield Plans, MD Anderson Cancer Center, Thibodaux Regional Hospital, University of New Hampshire, Commonwealth Health Corporation, Charleston Area Medical Center, Mount Carmel Health System and Bon Secours National Health System, just to name a few (see case studies chapters).
Six Sigma projects are defined as projects designed to reduce error rates to a maximum of 3.44 errors per million exposures (or “opportunities”) through the use of statistical analysis techniques, problem solving, and quality principles. The typical healthcare organization has error rates in excess of between 2,700 and 45,500 (3 and 2 sigma) errors per million opportunities. Individuals, departments, projects, functions, plants, or entire organizations can use the Six Sigma approach.
More important than the specific measurement of error rates (because healthcare is about people as well as process) is the methodology behind Six Sigma. The Six Sigma process forces hospitals to measure those things that are important to the business of healthcare, things like quality, mortality, customer satisfaction, and employee satisfaction. If a hospital says that it is a patient-focused organization, what does that mean? And if the organization claims to be patient-centered (or focused), then how does it measure “patient focused?” If the hospital says it can’t measure that, then it is it really important to them? Most organizations limit their measurement mechanisms to traditional accounting measurements, such as income and expenses, but medical mistakes are typically not measured and are generally underreported due to malpractice and the tendency to penalize and terminate individuals who report errors. (After all, one critical error can lead to the revocation of a practitioner’s license.) Under a Six Sigma methodology, the hospital will find ways to measure what is important to them by tracing and analyzing the things they value the most as they relate to the internal or external customer’s needs. Organizations that can’t measure what they say they value don’t really value what they profess to value. And if they can’t measure it, they can’t improve it!
While many healthcare organizations have attempted process improvement throughout the last 20 years, most have ended in disappointment. The discipline of the Six Sigma approach to quality through process improvement (as apposed to isolated quality attempts—such as inspection and post-mortem review of errors) is potentially the industry’s best opportunity to address lingering issues of quality and the resultant real costs that are added to any system when poor quality is the rule, rather than the exception.
“When you can measure what you are speaking about, and express it in numbers, you know something about it; but when you cannot measure it, when you can not express it in numbers, your knowledge is of a meager and unsatisfactory kind. It may be the beginning of knowledge, but you have scarcely, in your thoughts, advanced to the stage of science.”
—William Thomson, Lord Kelvin (1824–1907)
A Brief Explanation of Six Sigma
An ever-growing number of healthcare organizations are using Six Sigma to improve processes, from admitting to discharge and all the administrative and clinical processes in between. This adoption is driven by several factors including the need to improve the organization’s bottom line, eliminate medical errors, and position themselves for an imminent global consumer-centered healthcare revolution. Healthcare providers once enjoyed a respect by their customers that few institutions in the world enjoy. Then came continuous years of double-digit cost increases capped off by the Institute of Health report indicating that medical errors kill approximately 98,000 people per year in the United States. These mistakes can range from prescription errors to a failure to wash hands. Many healthcare consumers began to question why increasing costs did not equate to improved quality. Accordingly, the healthcare industry finds itself at a crossroads—to continue on the current path, which would lead to disaster, and or the other road, leading to potential redemption. Many organizations thankfully have chosen a path of redemption: Six Sigma.
A brief history of Six Sigma is helpful to a healthcare entity considering a Six Sigma initiative. The earliest quality initiatives were based on 100 percent inspection, a concept that would be impossible in a service-oriented environment such as healthcare. Because this was expensive and time-consuming, sampling plans were developed to define acceptable defect levels. Then in the 1970s, quality guru Phil Crosby established a program called zero defects. This program was an inspirational way of explaining to employees the notion that everything should be done right the first time, that there should be no failures or defects in the work output. In the healthcare world, a defect can be as benign as an unpaid bill or as serious as a medication error causing the death of a patient. Probably more critical than in any other industry, zero defects should be the order of the day in a patient encounter.
The zero defects concept was somewhat controversial because some quality experts felt it mainly focused on meeting internal design specifications. It did not focus on customer requirements or on continuous improvement. Many quality professionals disagreed with the concept because they believed that it was impossible to have zero defects all the time. These process-oriented professionals felt that process capability requirements were a better way of defining acceptable performance. But the U.S. government quickly embraced this concept, and it became the “in” thing to do for a number of years.
In the 1970s and early 1980s, organizations such as IBM released requirements that their process capabilities (Cpk) must reach a 1.40 level, or an acceptable corrective action plan needed to be in place before products could be shipped to their customers. IBM’s technical report entitled “Process Qualification—Manufacturing Insurance Policy”1 required that a process “plus or minus 4 sigma limit” must fall within the specification limit when the following are considered:
• Accuracy
• Precision
• Repeatability/reproducibility
• Variation/stability
• Linearity, or resolution
• Sensitivity
• Variation between similar pieces of equipment used for the same purpose
In the mid 1980s, Motorola’s president directed that all processes should have a tenfold improvement within a five-year period. This called for radical changes in the way processes within Motorola functioned, thus the creation of Six Sigma. This program set an objective for all processes to statistically perform at an error rate no greater than 3.4 errors per million opportunities. The real breakthrough in Motorola’s Six Sigma approach was that the Six Sigma concept was applied to all processes, not just the manufacturing processes. (Obviously, in hindsight, was the fact that general systems theory creates a relationship between nearly all the processes in an organization.)
To calculate the process performance, samples of the output were plotted on a histogram, and the standard deviation was calculated. Once the standard deviation and mean were calculated, it was easy to compare the Six Sigma calculated performance limit to the specifications and/or requirements, if the organization has defined its requirements for each process and each activity within the process. Of course, this was not the case for most non-production activities. As a result, organizations that undertake a Six Sigma program are forced into a major upgrading of their internal requirements and measurement system.
Once the process variation and mean performance are compared to the requirements, most processes fail to meet the Six Sigma requirements. Many non-production processes fail to even meet a ±3 sigma performance level (3 defects per 1,000, or 3,000 per million). To place this in context, a routine appendectomy might consist of 200 to 300 opportunities for error (hand and room washing, instrument sterilization, scheduling, pharmaceuticals, skills of surgeon, and so on), most non-critical, but many fatal. The non-critical are the most common and result in “nickel and diming” up the cost of care, while the well-publicized critical errors might result in malpractice or expensive corrective action, such as repeat procedures or infection, or death of the patient, each of which is extremely expensive to organizations in reputation and in dollars. In a fast-paced and variable environment, such as a hospital emergency room, one might expect dramatic fluctuations in the sigma performance level, but typically the deviations from the mean are not much greater than that found in an accounting office. This is true because the defects built into the system are generally consistent across time.
Six Sigma quality became popular immediately following Motorola winning the Baldrige Award in 1988. The information package that Motorola distributed to explain their winning stated:
“To accomplish its quality and total customer satisfaction goals, Motorola concentrates on several key operational initiatives. At the top of the list is Six Sigma Quality, a statistical measure of variation from a desired result. In concrete terms, Six Sigma translates into a target of no more than 3.4 defects per million products, customer services included. At the manufacturing end, this requires designs that accommodate reasonable variation in component parts but production processes that yield consistently uniform final products. Motorola employees record the defects found in every function of the business, and statistical technologies are increasingly made part of each and every employee’s job.”
Although Motorola called its program Six Sigma, Motorola only required that Six Sigma be applied to one point in time (Cp = 2) and allowed the process to perform at lower levels when the process drift is considered (Cpk). Table 3.1 relates the various levels of sigma to defects per thousand and per million.
Table 3.1. Quality Levels and Corresponding Number of Defects
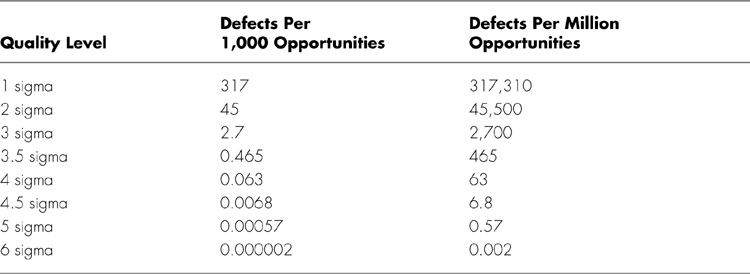
Note that our calculation differs from the 3.4 per million as defined by Motorola because we take into account the shift of process average.
Regardless of the specific measurement methodology used, a low sigma can result in consequences not traditionally identified in the normal course of business. For example, utilizing our Six Sigma measurement in the context of power company outages or misspelled words in a library, we see the data shown in Table 3.2.
Table 3.2. Defect Rate Versus Sigma Level for Power Outages and Misspelled Words
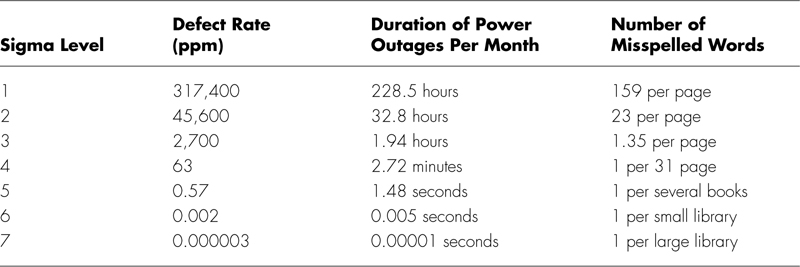
Although .002 errors per million fuses, bolts, screws, nuts, garden hoses, or brooms may not be an aggressive target, when you start to apply the same requirements to management decisions, drawings, books, letters, sales contracts, meals served, auto repairs, medical operations, sales calls, or lines of codes, it turns out to be a very aggressive target. This is particularly true in any type of service activity in which quality cannot be inspected or tested.
The Six Sigma program is not just a new performance standard because the new performance standard cannot be met if the organization does the same old thing the same old way. It is for this reason that Motorola calls its program the “Six Sigma Quality Program.” It drove a major improvement effort that radiated through the organization. Motorola’s Six Sigma quality program is shown in Figure 3.1.
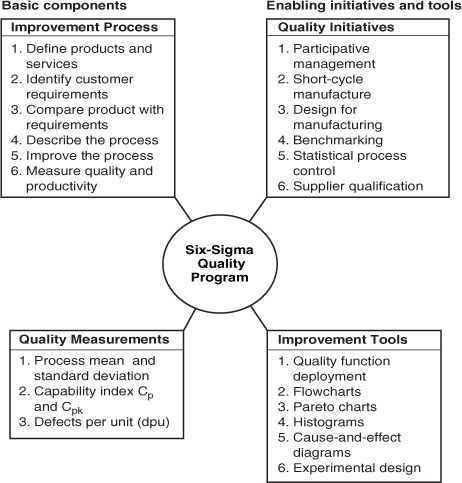
Figure 3.1. Six Sigma quality program
You will note that the Six Sigma quality program is divided into four major quadrants:
• Improvement process
• Quality initiatives
• Quality measurements
• Improvement tools
To help with the implementation of the Six Sigma quality program, Motorola formed the Six Sigma Research Center to develop a set of reference books known as the Encyclopedia of Six Sigma. This encyclopedia consists of three main parts:
• A collection of statistical tools
• Application case studies
• Descriptive, specific optimization methods
Motorola established an innovative recognition system, called the Black Belt program, to support the Six Sigma quality program. Individuals progress through various levels that were designated as:
• Green Belts. Individuals who have completed the training.
• Black Belts. Individuals highly competent to serve as the on-site consultants for applications of Six Sigma methodologies.
• Master Black Belts. Individuals who have mastered the Six Sigma process and are capable of teaching the process to others.
The following is a ten-step process to achieve Six Sigma in a clinically intensive process:
1. Identify Your Products. What is the service or product that you are producing? In the case of an operating suite, it might be technically superior procedures.
2. Identify Customer Requirements. What is the customer’s perception of error-free products or service? The response might be any adverse condition that would be deemed a medical mistake.
3. Diagnose the Frequency and Source of Errors. What is the source of errors? In an emergency department, errors could come from any number of places including supply carts or ineffective ambulance routing leading to overcrowded waiting rooms.
4. Design the Process. How can the process enablers be put together to provide a best-value solution? In said emergency room, perhaps some mechanisms can avoid the overcrowding.
5. Develop a Simulation Model. This model is used to project the process” performance characteristics and determine if the process will meet the customer’s error-free needs. Try a new scheduling system.
6. Error-Proof the Process. How can the process be changed to eliminate potential errors? In the operating suite, this might include new flow of personnel or redesigned procedure packs. In a billing department, this might include correction of mistakes by the admitting department.
7. Install Internal and External Control Points and Measurements. How can you detect trends before they become errors? In the case of the billing department, one might institute reporting of missing information or unsigned discharge orders before they reach final billing. In the case of the emergency room, correctly stocked supply carts might eliminate trips to and from Central Supply.
8. Install New Processes. How do you get the users to embrace the new process? (A pilot installation often is required. In any case, an early change management intervention is advised as is input by those affected.)
• Certify each step or activity in the process
• Qualify the total process as a single item
9. Measure Performance. Does the process meet the Six Sigma requirements? If not, how does the process need to be adjusted to do so?
10. Continuously Improve. How can the process” effectiveness, efficiency, and adaptability be improved?
To meet the very challenging quality requirements associated with Six Sigma, an organization has only three options: Reduce the process variability, center the mean of the population, or open the acceptable performance limit.
The first approach should always be to focus on centering the process mean and reducing the process breadth. Motorola’s research institute recommends the following six steps 2:
1. Identify the product characteristics that are critical to satisfying both the physical and functional requirements of the customer and the requirements of relevant regulatory agencies. This might mean that patients who come into your facility for a series of tests will have all of them performed on a single day rather than over an extended period.
2. Determine the specific product elements that contribute to achieving these critical characteristics. What does your organization do to streamline the process for the patient or coordinate appointments?
3. According to product elements, determine the process step or process choice that controls each critical characteristic. Is your organization designed to serve the staff, the equipment, the patient, or none of the above?
4. Determine a nominal design value and the maximum (real) allowable tolerance for each critical characteristic, which still guarantees successful required performance. How would you have to change the scheduling process to achieve the Six Sigma goals?
5. Determine the capability for parts and process elements that control critical characteristics. In the example of scheduling appointments in the same visit, is the limitation in IT systems, in physical layout of the plant, or is it rooted in outmoded processes?
6. If Cp is not = 2 (Cpk = 1.5), then change the design of the process to achieve Cp = 2 (or institute process control measures which will narrow process capability sufficiently to achieve Cp = 2). Note: Cpk is the process capability index and is referenced later in the book.
To make Six Sigma more personal, consider the case of a physician who performs more than 1,000 surgical procedures (1,000 opportunities for error per case) with no more than 1 mistake. Certainly, this is very challenging based upon normal performance levels. It requires a radical new design to the way the operating room functions.
A number of points need to be considered when you are using the Six Sigma process:
• Six Sigma works well where there are high production rates of the same or very similar parts. In other words, many organizations have tackled CABG (Coronary Artery Bypass Graft) since it fits the above requirement well.
• Six Sigma is very difficult to obtain in areas like administration, sales, personnel, and so on where results are difficult to measure and are unique from one incident to another.
• It is extremely difficult for management to perform at the Six Sigma level due to the high degree of variation in the “process” of managing.
• Six Sigma works well when variables data can be collected, but not so well when attributes data are used.
• It is based upon the use of normal distribution, not abnormal or skewed distributions.
Motorola defined a list of tools required to support the Six Sigma program. They are grouped into three categories: design, process, and material. These tools are easily adaptable to healthcare if you consider them from a slightly different perspective:
• Design Tools (or “Design of Care”)
• Design to standard parts/materials
• Design to standard processes
• Design to known capabilities
• Design for assembly
• Design for simplicity
• Design for robustness
• Process Tools (or “Process in Healthcare”)
• Short cycle manufacturing
• Process characterization
• Process standardization
• Process optimization
• Statistical process control
• Material Tools (or “Central/Sterile Supply Optimization”)
• Parts standardization
• Supplier SPC (Statistical Process Control)
• Supplier certification
• Material requirements planning
Why Do You Need Six Sigma?
Assume that a typical surgical procedure contains 1,200 processing steps (not unusual because the typical healthcare organization has approximately 20,000 individual processes). If each step has a short-term 4 sigma capability, the throughput yield would be (RT is rolled throughput yield):
YRT = 0.999968(1200) = 96.24%
If you consider over a period of time, the process drifts away from the nominal as much as 1.5 sigma, the yield at each step would be degraded to .9938 and the throughput yield would be:
YRT = 0.9938(1200) = 0.05%
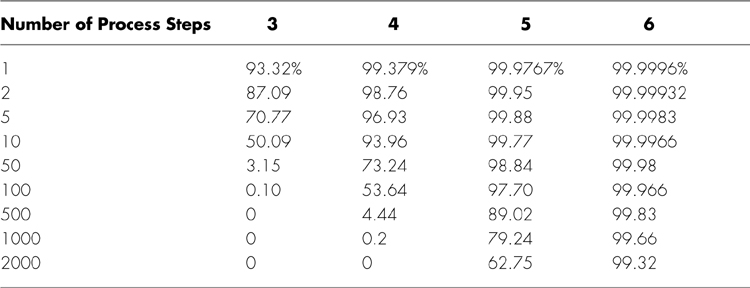
In other words, you have near zero possibility of completing a surgical procedure without committing an error. This is assuming that all the steps are in series with each other. Table 3.3 provides you with a breakdown of this concept based upon the number of steps in the process, and various sigma limits, assuming a 1.5 sigma shift.
Table 3.3. Throughput Yield Versus the Number of Process Steps and Processes
Quality
By applying Six Sigma principles, it is relatively easy to reduce current error rates, and a 50 percent reduction in errors in a 3 sigma healthcare organization cannot only lead to greater customer satisfaction, but large reductions in claims related to medical mistakes. The following sections describe some examples.
GE
Jack Welch launched the Six Sigma program at GE with 200 projects in 1995. In 1996, it increased to 3,000 projects. It expanded to 6,000 projects in 1997. The target for the Six Sigma program was to save $150 million in productivity gains and profits. The actual 1997 savings was $320 million, more than double the goal. In 1998, net savings were estimated to be about $750 million.
Some people within GE were concerned because they believed Six Sigma will cause bureaucracy to increase. Welch’s reply to this concern was, “I don’t give a damn if we get a little bureaucracy as long as we get the results.”
William Woodburn, head of GE’s industrial diamonds business, reports that in four years the operation’s returns on investment increased fourfold and, at the same time, the cost structure was cut in half. He gives the Six Sigma program credit for much of the improvement. To get the improvements, he had to cut more than a third of the workforce, which included more than 50 percent of the salaried staff.3
Allied Signal
Lawrence A. Bossidy, former GE Vice Chairman, started the Six Sigma program at Allied Signal Inc. when he was CEO in 1991. The increased productivity and profit got Jack Welch’s attention. At this time, GE was running at a 3 to 4 sigma level. The gap between 4 sigma and Six Sigma at GE was costing GE between $8 and $12 billion a year.
“There is one rule for Industrialists and that is: Make the best quality of goods possible at the lowest cost possible, paying the highest wages possible.”
—Henry Ford (1863–1947)
“I’m surprised we didn’t come up with this a few decades ago. For a hospital like ours, questioning and second-guessing is common.”
—Dr. George Kerlakean, Good Samaritan Hospital
Six Sigma Applied to Healthcare
The Six Sigma approach is in its infancy in the healthcare industry. It has been applied to some extent to refine some hospitals’ business processes using reengineering or process redesign methodologies. Monica Berry, president of the American Society for Healthcare Risk Management, stated, “If we look at quality as it has been implemented in the past, we won’t be successful in reducing patient errors.”
Most healthcare providers have put in place some type of Total Quality Management (TQM) or Continuous Quality Improvement (CQI) program. A Six Sigma project does not endanger these programs. In fact, it will enhance them as it builds on their strengths and puts additional focus on the measurement system.
The TQM programs focuses on defining the voice of both internal and external customers, Process Control, Process Redesign, Problem Solving (PDCA), teams and the need for objective data, total organizational involvement, and reporting in order to improve the processes.
The Continuous Quality Improvement model was defined in 1987 in the American Society for Quality book, The Improvement Process.4 It defines the continuous improvement process in the following 10 building blocks.
1. Obtain top management’s commitment.
2. Establish an improvement steering council.
3. Obtain total management participation.
4. Secure team participation.
5. Obtain individual involvement.
6. Establish system improvement teams (process control teams).
7. Develop supplier involvement activities.
8. Establish a systems assurance audit activity.
9. Develop and implement short-range and long-range improvement plans, and implement short-range strategy that will eliminate and prevent errors.
10. Establish recognition and reward systems that reinforce desired behaviors.
The system approach required cross-functional teams to be formed to work on process problems. For example, to reduce medication errors in a hospital required a team made up of delivering nurses, ordering physicians, dispensing pharmacists, and medication suppliers, all working together. At Stanford Hospital, they formed 11 cross-departmental teams. For example, the Cardiac Surgery team was made up of the following members:
• Physician champion/Co-Leader
• Department manager/Co-Leader
• Clinical specialists
• Pharmacists
• Social workers
• Case managers
• Respiratory therapists
• Managers from all the process departments
• Clinical financial analysts
• A consultant
The measurement system for the CQI approach was called “Poor Quality Cost,” as defined in ASQC’s improvement in reduction in the cost of the following:
• Prevention cost
• Appraisal cost
• Internal error cost
• External error cost
• Test Equipment cost
• Customer-incurred cost (resulting from errors)
• Customer-dissatisfaction cost
• Loss-of-reputation cost
• Last opportunity cost
Note that in the 1980s, the CQI approach was directed at reducing cost caused by errors. This changed in the 1990s as cycle time became as important in many cases, sometimes more important than cost.
The problem-analysis cycle was called “The Opportunity Cycle” and consisted of five phases:
• Phase 1 - Problem Selection
• Phase 2 - Root cause Analysis
• Phase 3 - Correction
• Phase 4 - Measurement
• Phase 5 - Prevention
Many organizations just stayed with the old, proven Shewhart (or Deming) cycle because it was simpler. It consists of the following:
• Plan. What to identify or accomplish.
• Do. Initiate the strategy or plan.
• Check. Evaluate the outcome of the strategy or plan.
• Act. What have we ascertained?
Another quality model sometimes used in healthcare was developed by a well-known physician, Dr. Avedis Donabedian.
The Donabedian model developed in the 1980s focused on three domains:
• Structure
• Process
• Outcome
You will note that all three approaches have a focus on processes such as the following:
• Pharmaceutical care
• Diagnostic testing
• Accurate drug administration
• Registration
• Billing
• Appointment scheduling
It is easy to see that the Six Sigma approach should blend easily with your present quality system and improve upon it. It is a normal addition to your current system to help update it with the best and latest proven technology.
Six Sigma at Work in Healthcare
Some healthcare units are running pilot Six Sigma projects, and the results are very encouraging.
Typical improvements are
• Reduced length of stay
• Improved customer satisfaction
• Reduced time to enter the healthcare unit
• Reduced inventory
• Increased efficiency in the billing system
Typical Six Sigma activities include the following:
• Charleston Area Medical Center applied Six Sigma to its supply chain management for surgical supplies saving $1 million.
• Virtual Health focused on its congestive heart failure patients and reduced variation leading to shorter length of time to recover.
• Scottsdale Healthcare applied Six Sigma approaches to the emergency room process and reduced the time required to transfer a patient to an in-patient hospital bed, increasing profits by $1.6 million per year.
“We do this project so that our staff learns and achieves results by proactively participating in the Six Sigma process. The result (decline) in registered nurse overtime alone was 65 percent over one year.”
—Douglas Sears, Bon Secours Health Systems
“The results were a reduced average ventilators length of stay of 25 percent and reduction of defects per million opportunities by 12 percent for annualized savings of $450,000.”
—Sarah Davis, Director of Nursing, Sentara
• One of the Stanford Hospital and Clinics’ Six Sigma teams directed the Coronary Artery Bypass Graft (CABG) Surgery process. The results were outstanding:
• Annual savings of $15 million (U.S.)
• The mortality rate dropped from 7.1 percent to 3.7 percent for all CABG procedures
• Costs were reduced by 40 percent
• Intensive care time was reduced by 8 hours
• Intubation time was reduced from 12–16 hours to 4–6 hours
• Theresa Garrison reports that at St. Louis Hospital, they were able to reduce infections by 65 percent.
• Hospital with good team spirit and nurses with authority to act on their own in case of sudden problems had 59 percent lower than average death rates.
• Stanford Hospital and Clinic saved $25 million per year from standardized purchasing and other process improvements.
Six Sigma will help in many ways. It is not just a problem-solving tool; it is also an information gathering and analysis tool. There is a huge information gap. The present data systems in most hospitals are poor at best. Therefore, doing any Six Sigma project in the typical healthcare setting can prove to be difficult and time consuming.
Because the typical healthcare project requires more manual information gathering (observations, stop-watch exercises, walk-through) than the average manufacturing organization we often find that this is the true “moment of truth” for the healthcare organization. For example, if one wants to track the time it takes to go through the admissions process in the typical hospital, the Six Sigma practitioner will likely find that the information isn’t available or is only available without the granularity that is necessary to create a sound hypothesis. Because data collection can be expensive and time consuming and there are so many information voids in the typical healthcare organization, many give up the Six Sigma effort at this point (or the effort languishes in a near-completion state).
At this point, the enlightened organization redoubles its efforts to capture valuable information for the current and future studies (as well as SPC). While we do not know the actual number of times Six Sigma efforts are abandoned at this critical state, we have seen it happen far too many times and, just as the road to the Ph.D. is strewn with unfinished dissertations, so is the road to the Black Belt. This is one of the most important reasons for following the implementation guidelines from later in this book to a tee, as well as finding a champion or MBB who has not only been a part of a Six Sigma program, but one who has actually started a program and has executive presence and strong leadership skills.
Vicky Gregg from Blue Cross Blue Shield of Tennessee, when he was discussing the quality and quality of outcome information that was available to the customers, stated, “If you think about it as the equivalent of a manufacturer not having the system and information flow to understand and measure quality, that’s pretty scary.” The Six Sigma approach to data collection analysis can help with this problem along with electronic record keeping.
Six Sigma also attacks the basic problem that all hospitals have: the variation in the way things are done. For example, a simple urinary tract infection without any complications can be treated in 135 different ways. Which process provides the best overall value? No one knows or everyone would be using it.
Training is a key part of preparing the organization for Six Sigma. The following is the minimum Six Sigma training required by job assignment based upon ASQ (American Society for Quality) recommendations:
• Executive: one day overview
• Upper Management Champions: 5 days
• Six Sigma Green Belt: 10 days on Six Sigma concepts
• Six Sigma Black Belt: 20 days during a 4-month period
Most organizations do all of the above in half the time and will heavily focus the training on field experience and improvement projects.
Different Views of Healthcare Quality
One of the problems that slow down quality in healthcare is the many different views of what quality is. For example,
• The paying organization views quality as a measure of the value associated with the delivered care.
• The physician/nurse views quality as making the right diagnosis, prescribing the right medicine, and employing the right procedure to make the patient better. It’s doing the right job from a scientific point of view.
• The patients view quality as the perceived services, such as: Are the employees gracious? Do they appear to be competent? Are they receiving timely care? Is the hospital a good environment?
• The healthcare managers view quality as the appropriateness of care. Quality in healthcare is the evaluation of the appropriateness of treatment.
When we develop the healthcare system, all four views of quality must be designed into the system.
Conclusions
Many other non-healthcare organizations have embraced the Six Sigma concepts. Among them are IBM, Texas Instruments, Defense System Electronics Group (DSEG), and GE. While the implementation of Six Sigma in a healthcare-provider setting is in its early stages, some of the top healthcare organizations in the world are interested in the possibilities. Most quality-focused organizations performed at the 4 sigma level at the beginning of the 1990s. As of this date, we know of no organization that is performing all of its measurements to the Six Sigma requirements. Our experience indicates that Six Sigma and the related methodologies are not implemented without difficulties.
G. Don Taylor and John R. English, in their paper entitled “A Benchmarking Framework for Quality Improvement,”7 point out the five following problems related to the Six Sigma methodology:
• Determining how to measure defects
• Applying Six Sigma in non-traditional settings
• Determining whether to relax specifications or to reduce the normal variability of the product
• The use of restrictive assumptions
• The determination of appropriate tools to use to achieve Six Sigma goals
Motorola, on the other hand, reports the following results (in a manufacturing environment):
• Improved yields and lower than expected fallout during manufacturing (this could equate to less use of supplies or less errors)
• Better productivity
• Higher performance
• Improved MTTF (Mean Time To Failure)
• Lower manufacturing cost (or lower costs per procedure, patient, and so on)
• Improved customer satisfaction
GE has embraced the Six Sigma concept in order to drive its future quality improvement activities. GE’s Six Sigma program is the largest quality initiative ever mounted in the U.S. They call their design for Six Sigma DMADV, which stands for:
• Define. Define the process, product or service that will be improved. Define the customer’s view of error-free performance.
• Measure. Evaluate the current item’s performance.
• Analyze. Define best practices, benchmarks, and enablers.
• Design. Develop a best-value future-state solution.
• Verify. Measure the new item to ensure it meets the requirements documented in the define stage and the Six Sigma requirements.
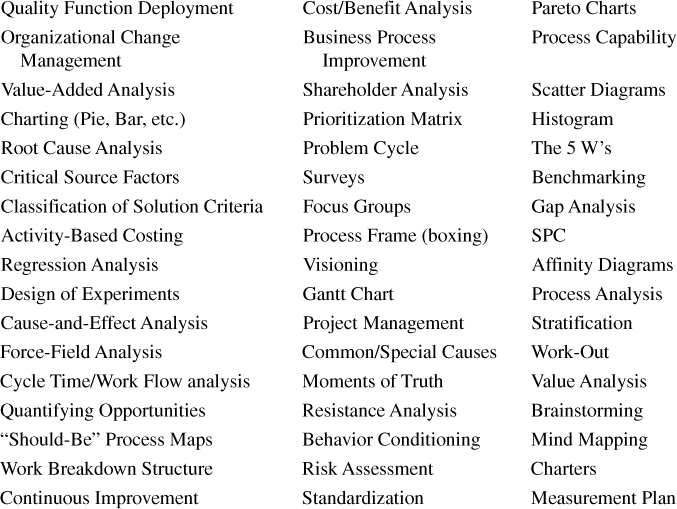
As an example, the following are a few of the tools and techniques used by GE in support of Six Sigma:
It is very important to point out that one of the most used tools in Total Six Sigma is Business Process Improvement (BPI). The three major methodologies that are included in BPI include the following:
• Process redesign
• Process reengineering
• Process benchmarking
All three require that a very effective change management project is used in conjunction or the possibility of failure runs very high.
Hammer and Champy in their book, Reengineering the Corporation, reported, “Some 50 to 70 percent of reengineering attempts fail to deliver the intended dramatic results.”8
Six Sigma Potential in Healthcare
So, where can a healthcare organization find Six Sigma opportunities? It’s clear in manufacturing where opportunities lie, but in the healthcare space we are talking about service, we are talking about mass customization, and we are talking about customer/patient lives.
In fact, there are almost limitless opportunities in healthcare. Most Six Sigma practitioners find that services in general, and healthcare in particular, are some of the most fertile ground available. These opportunities generally come in from a wasteful and inefficient administrative process but can just as easily be found in the clinical space and, amazingly enough, in the hands of the patients. In no other business is the vested interest as great as in the healthcare space. Patients and families are more than happy to participate in any effort to reduce variation and potentially adverse outcomes.
Some examples of where Six Sigma might work in healthcare could be
• Billing Department. Imagine a billing department that reduced errors in processing patient bills to a 5 sigma process level. While the department might be producing claims at a very efficient and effective rate, it is common knowledge in the industry that many claims are rejected due to errors by personnel at the payer organization. As of Fall 2003, Cigna, Anthem, and many of the Blues are implementing Six Sigma in their organizations. Should a provider and payer agree to implement Six Sigma in tandem, tremendous savings could be achieved solely on the potential to reduce or eliminate claims adjudication in favor of a “trusted” claims chain.
• Emergency Department. Imagine an emergency department with a phone-in triage function aimed at “pre-processing” patients for the appropriateness of care. Six Sigma could enable an Emergency Department to send potential ER department patients to more appropriate venues of care or sister facilities for load balancing—a not unheard-of application when most patients could use their cell phones to call on-route.
• Floor Procedures. Imagine a system where patients gain control of their stay via meal delivery as a “menu with room service.” This psychological “control” leads to faster recovery times, increased patient satisfaction, and potential reduced costs by the food services department through better balancing food preparation throughout the day instead of centered on breakfast, lunch, and dinner.
What would work in one facility wouldn’t necessarily work in another, and this is the beauty of the Six Sigma approach. Instead of following the cookie-cutter approach of the healthcare provider down the street, the hospital is able to evaluate its own opportunities and work to improve its unique opportunities. Just as facilities specialize, so too are they empowered by the Six Sigma process to individually identify and improve processes tailored to their individual patient population, payer mix, and staffing situation. Six Sigma truly offers an opportunity for a breakthrough in healthcare.
In the past, we have believed that the healthcare system was too complex with too many players—companies, insurers, medical device makers, pharmaceutical companies, doctors, nurses, hospitals, special interest groups, and others—to actually gain control over a process, never mind a system. These players all have different interests and objectives and, in fact, different motivations for correcting the problem. But if we, the business community, do not step up to the challenge, the government will have to and we believe we can find a better answer. Now, Six Sigma is not the total answer to the problems we are facing in our healthcare system, but it can be a key part. It is time to start making some major changes.
Healthcare organizations may be the type of service organization for the use of Six Sigma. If one considers the very nature of the business, one might notice that in fact healthcare is generally a highly repetitive environment, subject to variation in disease from patient to patient, yes, but generally uniform in the reaction to the variation by patient. While Patient A might require a different dose of a medicine than Patient B in response to an episode, the common factors would be method of ordering and delivering the medication, administering, and documenting the incident. The staff and physicians would be the same—the pharmacy, the crash carts, the floor layouts all generally the same. The only thing that might vary is the patient’s reaction to the drug in question at the dose administered. In fact, one could argue that the “practice” of medicine is actually not what we do on the average patient, but what we do in the exception—the day-to-day treatment of our patients is the science of medicine, and science requires a scientific approach to the delivery of medicine. Six Sigma is as close to scientific management than anything that has come before.
Consider the scientific method. One definition we like is “principles and procedures for the systematic pursuit of knowledge involving the recognition and formulation of a problem, the collection of data through observation and experiment, and the formulation and testing of hypotheses.”9 In respect to the methodology of Six Sigma, which we will discuss in greater detail later in the book, Six Sigma allows for:
• Principles and procedures for the systematic pursuit of knowledge; knowledge being about critical to quality characteristics and the understanding and measurement of said characteristics.
• Involving the recognition and formulation of a problem, as formulated in the Six Sigma project charter specifically addressing the problem we will try to solve, the magnitude, and the risks involved.
• The collection of data through observation and experiment, and the formulation and testing of hypotheses, as manifested in the collection of data, development of hypothesis, testing of hypothesis, and development of tests of the hypothesis.
In addition, Six Sigma allows you to utilize the scientific method to actually apply the improvements for immediate benefits to your patients, their families, and the overall well being of the healthcare organization. Accordingly, Six Sigma fits so well with the culture and environment of healthcare that it is one of the most logical and effective extensions of healthcare to come along in the last 50 years.
Medicine, Measurement, and Science
The current healthcare error rate in the U.S. is about 6,210 errors per million opportunities (3.8 sigma) and for some treatment activities runs as high as 1 sigma. Compare this to the manufacturing Six Sigma standard of 3.4 errors per million opportunities for all processes.
According to Altman, at least 150 times since 1996, surgeons in hospitals in this country have operated on the wrong arm, leg, eye, kidney or other body part, or even on the wrong patient.10 The figure does not include near misses, such as when doctors have started to operate on the wrong part of the patient or even the wrong patient, but stopped before the operation was completed because the error was detected. No one collects such information.
Complex Business
Thirty to forty percent of the cost waste is caused by errors made by specialists.
The U.S. government estimates that IT can save $140 billion per year through improved patient care and the elimination of redundant tests ordered.
In September, 2003, Tawnya Brown underwent surgery at Inova Fairfax Hospital in Falls Church, Virgina. Although the surgery went well, the patient ultimately died. Brown was given two pints of A-negative blood and her blood type was O-positive. To make the condition worse, her doctor called for more blood when he discovered that she was not doing well in recovery. In the following three hours, she received six more pints of the wrong type of blood. (A person her size can hold a volume of about eight pints of blood only.) The day before the surgery, a technician drew a blood sample so that the correct type would be available if needed. The problem was that the technician took the sample from the wrong patient. This should have been discovered by the phlebotomist, but he failed to perform two required identification screens: checking the patient’s hospital bracelet and asking the patient to state her name. The financial settlement for this error was about $1.7 million. But not even $1.7 million can make up the loss of a mother to an eight-year old girl.
Brian Bachman, two years of age, died after undergoing a liver transplant at the Fairview University Medical Center in Minnesota. The surgery was uncomplicated, and Brian was doing well initially. However, two days after the surgery, Brian’s condition worsened. At 7 a.m., a nurse misread the table on a log of Heparin she was replacing. The new bag contained a much higher concentration of blood thinner than the one she was replacing, and the machine delivering the medication was not reprogrammed. Brian began receiving 10 times the amount ordered by the physician. The staff failed to notice the mistake throughout the day, even though the medication drip was checked every 15 minutes. The error was finally discovered by the evening nurse, but Brian had already experienced internal bleeding and a blood clot in the artery leading to his liver. A blood clot can trigger liver damage, which can cause swelling of the brain and brain death. Doctors determined that the little boy “will most likely remain in a vegetative state.” As a result, Brian was taken off life support and died soon thereafter. Mike Sertz, Fairview’s Vice President for Risk Management, stated, “It was more a system error than an individual error.”
Fraud and Abuse
Healthcare costs run $1.7 trillion a year. Fraud and abuse run between $50 and $75 billion a year. In controlling variation, fraud and abuse can be more easily identified and dealt with.
Six Sigma can be a great tool in fighting healthcare fraud and abuse. For example, billing for services not furnished is arguably the single most common method of deceiving or misrepresenting services delivered. Because Six Sigma utilizes statistical process control as a core tool, variations in standard practice will always be noted. Too many treatments, too many supplies, or too many visits will, by definition, signal the system to investigate the reasons for the variation. This argument can also be made for unbundling or “exploding” charges, and “upcoding.”
Another typical healthcare fraud and abuse practice is the misrepresentation of a diagnosis, which can be identified through controls when individual institutions or physicians seem to consistently have sicker patients than the population in general. This argument also works in the case of falsification of certificates of medical necessity, plans of treatment, and medical records.
Only by gaining a true understanding of your healthcare business can you begin to get a real handle on the indicators of fraud and abuse. Six Sigma enables you to spot outliers before they become a big problem for the provider.
Dedication to Perfection and Elimination of Errors
Each year an estimated 1,500 surgical patients have foreign objects (such as sponges) left in them during surgery, leaving many to face crippling health problems. However, there is no mandatory system for reporting errors, leaving the actual number of medical errors in question.
It is often only through malpractice lawsuits that these errors become public knowledge. The article goes on to report that 5 percent of doctors are found responsible for more than 50 percent of successful malpractice suits. One caution: Most malpractice cases don’t make it to court. Only one in six victims even file, and about half of those abandon the effort before trial.11
Performance
Contrary to popular belief, effective performance metrics in healthcare are virtually nonexistent.
Hospitals with an atmosphere and/or culture of distrust have a death rate that is 58 percent higher than average.
Ramon Cruz, 81, had not even been hospitalized when Good Samaritan Hospital Medical Center in Islip, NY, forwarded the incorrect information to government agencies that he had died. Apparently, a hospital worker called up the wrong “Ramon Cruz” in the database. Cruz’s monthly Social Security checks were halted, his bank accounts emptied, and Medicare benefits terminated. A spokesman said all Cruz’s lost money will be returned, adding that it would take a couple of months.12
Customer Focus
According to the Centers for Disease Control, two million patients per year acquire an infection in the U.S. when hospitalized for conditions not related to the infection, and 88,000 die as a direct or indirect result. This adds an additional healthcare cost of $5 billion.13
According to the CDC’s William Jarvis, MD, and scientific chair of the healthcare-associated infections conference sponsored by CDC, “If you get an infection while you’re in the hospital for an operation for heart disease, for example, your hospital stay may be extended by days, and sometimes weeks, before the infection is cured.”
In general, the number of extra days a patient has to spend in the hospital varies depending on the type of infection he or she gets: an estimated 1 to 4 days for a urinary tract infection, 7 to 8 days for an infection at the site of a surgery procedure, 7 to 21 days for a bloodstream infection, and 7 to 30 days for pneumonia.
“The costs vary, too,” Dr. Jarvis said. “Anywhere from $600 or so for a urinary tract infection to $5,000 or more for pneumonia. Prolonged bloodstream infections can top $50,000.”
According to some experts, a patient improves faster at home by 10 to 60 percent than in a healthcare facility.
Complaints about hospital bills are as common as complaints about hospital food. Consumer Reports recently surveyed 21,000 readers on satisfaction with hospital stays. Of the 11,000 respondents who had reviewed their itemized hospital bills, 5 percent said they found major errors. Respondents with out-of-pocket expenses of $2,000 or more were twice as likely to have found billing errors.14
Consumerism in healthcare is another hot topic. Health Savings Accounts were introduced in 2005 to mixed reviews. Since then, they have been growing in popularity with employers and insurers. While some might be advocating a repeal of the law, the plan, which allows customers to opt into a high deductible health plan while investing their own money in healthcare expenses below the deductable, is proving to be popular.
What this means to the healthcare provider is that customers/patients now have a say in how, where, and with whom they will spend their money. It is doubtful that customers will spend their discretionary money at healthcare organizations that cannot or will not invest in quality and customer-focused care.
Staffing Shortages
There is a critical shortage of nurses. This is caused by several factors, including
• A growing demand as the baby boomers retire.
• The high cost of training a nurse. Because many universities find that tuition stratification is difficult (that is, charging different amounts based on the major), classes and majors that require labs, small classes, and highly skilled instructors are not as profitable as others.
• A nursing instructor with a Masters degree is paid less than half that of a hospital nurse. Given the pay differential, universities are finding it very difficult to recruit nursing professors.
• Finally, nursing can be difficult and sometimes hazardous. In general, the hours are long, the work is dirty, and the pay is less than a comparable position outside the hospital. Accordingly, many nursing professionals leave the field each year for easier work at software companies, pharmaceutical companies, and doctors’ offices.
Patricia Ann Hottois, age 53 of Phoenix, died of septic shock after the abdominal pad was left in her surgical wound. She had her surgery on June 8, 2003, at Maricopa Medical Center. About two weeks after the surgery, she was still complaining about the pain when her doctors discovered that the pad was left inside her. She died on July 1, 2003. This medical malpractice case was settled for $320,000.15 These types of errors should be eliminated by just doing a sponge count. According to a 2003 study in the New England Journal of Medicine, this type of surgical error occurs in about 1 out of every 1,000 to 1,500 abdominal operations, a lot more than the six sigma goal of 3.4 per million.
On March 19, 2004, two patients died at Foothill Medical Centre because they got an incorrect solution during dialysis treatment. They were given a potassium chloride solution instead of sodium chloride. The mix-up took place in the hospital’s pharmacy. Dr. Bob Johnston, the CHR’s Chief Medical Officer, stated “Despite our best efforts, errors do occur.” Barry Cavanaugh, Chief Executive of the Pharmacists Association of Alberta, stated, “An adverse event could happen because they are overworked.”16
Costs to Society
In the U.S., healthcare accounts for 15 percent of the GNP, and it will continue to rise to 18 percent. This compares to 8 percent and 10 percent in developing regions such as Japan, Europe, and Canada.
Two percent of hospital patients experience an adverse drug reaction, resulting in an increased length of stay and $4,700 added needless expenses. This accounts for 2.5 percent of the hospital’s budget.17
One person in the U.S. dies every eight minutes as a result of nosocomial infection, and 95 percent are preventable.18
About 20 percent of U.S. “products and services” extra cost is caused by our legal system.19
“Survey: 40 percent of public experienced medical errors,” which appeared in the New England Journal of Medicine, reports that more than one-third of practicing physicians and 40 percent of the public have experienced a medical error in the care that they or a family member received as patients. One of the findings of the survey is that “physicians disagree with national experts on the effectiveness of many of the proposed solutions to the problem of medical errors.”20
Endnotes
1. Harrington, H James. “Process qualification manufacturing insurance policy.” IBM Technical Report, September 15, 1980.
2. Coppola, Anthony. Six Sigma Programs. DoD Reliability Analysis Center START Sheets, 1990. Volume 6, Number 5.
3. Byrne, John A. “How Jack Welch Runs GE”. BusinessWeek, June 9, 1998, p. 47.
4. Harrington, H. James. The Improvement Process. (McGraw-Hill, 1987).
5. Cutler, A.N. (2001, August 22). http://www.sigma-engineering.co.uk/, Sigma Engineering Partnership.
6. Trusko, Brett E. (2006, November 14). http://www.jointcommission.org/Codman/Avedis_Donabedian.htm, Ernest Emory Codman Award.
7. Taylor, G. Don and English, John. “A Benchmarking Framework for Quality Improvement.” Quality Engineering, Vol. 6, No. 1, July 1993, pp. 57-69
8. Hammer, M and Champy, J. Reengineering the Corporation: A Manifesto for Business Revolution (New York: Harper Business, 1993).
9. tangents.home.att.net/data/rlgdef.htm.
10. Altman, L.K. “The wrong foot, and other tales of surgical error,” The New York Times, December 11, 2001.
11. Burton, Susan. “The Biggest Mistake of Their Lives,” The New York Times, March 16, 2003.
12. Associated Press. “Government Declares Man Very Much Alive, Dead.” Associated Press, February 19, 2002.
13. Centers for Disease Control (United States). Hospital infections cost U.S. billions of dollars annually. Media Relations. Monday March 6, 2000. http://www.cdc.gov/od/oc/media/pressrel/r2k0306b.htm.
14. Consumer Reports, 2003. “Decoding your hospital bills. You can find and fix costly errors.”http://www.consumerreports.org/cro/personal-finance/decoding-hospital-bills-103/overview/index.htm.
15. Leonard, Christina. “Surgery Mistake Is Costly,” The Arizona Republic. June 25, 2004.
16. Trusko, B and Harrington, H.J., “The Prescription for Health Care Excellence - Take Six Sigma As Needed.” Quality Digest. http://qualitydigest.com/IQedit/qdarticle_print.lasso?articleid=8889&-session=ACCESS:40A788221b3f61DA5DynTy16AE15. 2006.
17. Institute of Medicine. Preventing Medication Errors: Quality Chasm Series. July 20, 2006.
18. Centers for Disease Control (United States). Hospital infections cost U.S. billions of dollars annually. Media Relations. Monday March 6, 2000. http://www.cdc.gov/od/oc/media/pressrel/r2k0306b.htm.
19. Council of Economic Advisors. Who pays for tort liability claims? An economic analysis of the U.S. tort liability system. April 2002.
20. Davis, Robert. Survey: 40 percent of public experienced medical errors. Asbury Park Press, December 15, 2002.