Chapter 9
The Sensory Defensive Child: When the World is Too Bright, Noisy, and Too Close for Comfort
Abstract
Many children suffering from mood dysregulation show symptoms of sensory defensiveness. It is very common for children with these difficulties to become extremely agitated when touched by others, irritated by certain kinds of clothing on their body, or angry if bumped in a crowd. Often children with tactile hypersensitivities have difficulty developing close relationships with others—both emotionally and physically. Other sensory channels can be compromised as well. The child may experience sensory overload from being subjected to random or intrusive noises in the environment and avoid situations or interactions with others for this reason. Visual clutter or bright lights may be highly disorganizing especially if the child has attentional problems. Or the child may be extremely fearful of movement to the point that they resist exercise or sports, and avoid places that challenge their balance. A very common attribute of such individuals is a strong tendency to becoming highly disorganized and overwhelmed when there is too much overall stimulation in the environment and too many activities in a short period of time. “Less is better” should be their mantra.
Keywords
sensory integration
sensory modulation disorder
sensory channels
tactile defensiveness
gravitational insecurity
Many children suffering from mood dysregulation show symptoms of sensory defensiveness. It is very common for children with these difficulties to become extremely agitated when touched by others, irritated by certain kinds of clothing on their body, or angry if bumped in a crowd. Often children with tactile hypersensitivities have difficulty developing close relationships with others—both emotionally and physically. Other sensory channels can be compromised as well. The child may experience sensory overload from being subjected to random or intrusive noises in the environment and avoid situations or interactions with others for this reason. Visual clutter or bright lights may be highly disorganizing especially if the child has attentional problems. Or the child may be extremely fearful of movement to the point that they resist exercise or sports, and avoid places that challenge their balance. A very common attribute of such individuals is a strong tendency to becoming highly disorganized and overwhelmed when there is too much overall stimulation in the environment and too many activities in a short period of time. “Less is better” should be their mantra.
1. What is sensory integration?
All of us have an inner drive for sensory integration. It is the capacity of the central nervous system to integrate information from the various senses to enable the person to interact with the world. It allows the person to tolerate a range of sensory experiences and to integrate information from the various senses for self-calming, attention and learning, coordinated movement, and purposeful interactions with the world of things and people.
An important aspect of sensory integration is a process called modulation. This is when the nervous system balances the person’s level of arousal with the intensity of stimulation being experienced. It is the body’s own internal thermostat that cues us when to rouse or to calm oneself. For instance, if one feels sluggish, the person may exercise, chew gum, or listen to rock and roll music to increase their arousal level. When a child has sensory integrative problems, he or she does not have this internal capacity to modulate level of arousal. For example, after a stimulating day with many activities, the child may come home and begin to jump on the bed and run up and down the stairs, not feeling in the least bit ready to fall asleep at bedtime.
There are a wide range of skills that encompass the area of sensory integration that change as the child develops. During the first 2 years of life, the infant learns to detect and interpret information from the senses. The most important sensory channels at this stage of development are the basic senses of tactile or touch, vestibular or movement, proprioception or position in space of limbs, vision, and hearing. The infant uses information from these senses to develop coordination of the two body sides, to develop basic posture and balance, fine and gross motor skills, such as walking and using a refined pinch, and basic body scheme. Not only that, but these basic senses of touch, movement, and proprioception are encoded into relational experiences and impact how we interact and view the person world. Being touched, held, and moved by others are encoded by these basic sensory systems.
For the young infant, sensory integration occurs in the context of everyday routines and experiences. For instance, when the baby is touched, dressed, or bathed, they learn about their body and that touch can be a pleasurable experience with a loving caregiver. Some infants learn that different sensory experiences are coupled with each parent. For example, when the baby sees her father, she may squeal gleefully in hopes of rough housing time, yet she likes the holding and cuddling that her mother gives her as she nurses or look at picture books. Parents provide different experiences based on their own knowledge, experience of the world, and their own sensory preferences. Over the course of a person’s life, we associate certain sensory experiences with certain persons. These experiences can have a profound impact on the quality of the person’s attachment. For example, if a child has a caregiver who is neglectful or abusive, the child will engage in avoidant behavior as much as possible when in the caregiver’s presence.
The basic skills learned in infancy become more refined in the preschool years. The child learns how to coordinate both hands in skilled activities, such as scissor cutting and buttoning and to coordinate both sides of the body in activities, such as jumping or riding a tricycle. Motor planning develops so that the child can imitate and organize sophisticated sequences of movement, such as climbing up a jungle gym, swinging on the trapeze bar, then sliding down the slide. The preschool child also learns to combine sensory and motor skills for learning. For example, vision and movement are integrated for tasks, such as puzzle completion, sorting and stacking cups, and tracing shapes. As the child grows older, these skills may involve dancing, sports, skilled crafts, and the ability to enact complex projects from start to finish.
By the school-age years, there is continual refinement of sensory discrimination, integrating information from two or more senses. For example, the child can identify shapes by feel (stereognosis) or replicate shapes drawn on the back of his hand (graphesthesia). These skills help in the development of more complex perceptual skills, such as learning to read and write. By the age of 9–10 years, the process of sensory integration should be accomplished.
The earliest descriptions of sensory integration dysfunction were provided by Ayres (1972). Through her ground-breaking research, Dr. Ayres identified specific types of sensory integrative dysfunction (Ayres, 1985; Ayres, Mailloux, & Wendler, 1987). She has helped clinicians and researchers to understand the manifestation of sensory integrative disorders and their treatment. Much of what will be described in this chapter is based upon Dr. Ayres’ original work and those who have followed in her footsteps. Emphasis, however, is placed upon the impact of sensory processing disorders on the parent–child relationship and the child’s social and emotional functioning.
This chapter will describe sensory integrative disorders in infants and children and their treatment. The first section focuses on the various types of sensory integrative dysfunction. The following sections will highlight common sensory integrative problems in children and how they are treated. Case examples are presented to illustrate key points. Two in-depth cases are described that demonstrate how sensory integrative therapy is blended with both structured and child-centered therapy approaches with a child with pervasive developmental disorder (PDD) and in a longitudinal case of a child with nonverbal learning disability, spanning the course of her treatment from infancy to adulthood. These two cases were selected because many children with these disorders show significant sensory integrative dysfunction while struggling with the process of social engagement.
2. Sensory integrative dysfunction
Sensory integrative disorders have been documented among children and adults with learning disabilities, autism, and schizophrenia (Kinnealey, Oliver, & Wilbarger, 1995; Heller, 2003). It has been estimated that approximately 70% of learning disabled children have sensory integrative disorders (Carte, Morrison, Sublett, Uemura, & Setrakian, 1984). Developmental dyspraxia, a disorder involving the sequencing of motor actions is the most common type of sensory integrative disorder, occurring in about 35% of these children (Schaffer, Law, Polatajko, & Miller, 1989). Deficits in the processing of vestibular and tactile information are common among children with learning disorders and motor incoordination (Ayres, 1972; Chu, 1996; DeQuiros, 1976; Fisher, Mixon, & Herman, 1986; Horak, Shumway-Cook, Crowe, & Black, 1988) and in autistic children and schizophrenic adults (Maurer & Damasio, 1979; Ornitz, 1970; 1974; Ottenbacher, 1978). In addition, sensory processing dysfunction has been identified in postinstitutionalized children (e.g., Romanian orphanages) who have suffered sensory deprivation (Cermak & Daunhauer, 1997).
Persons suffering from posttraumatic stress disorder at any age can develop sensory defensiveness. Other causes of sensory defensiveness can be induced by a head trauma or incidents of physical, sexual, or psychological abuse. And individuals who engage in substance abuse may create a state of sensory defensiveness, even when they might be seeking to self-treat their internal state of dysregulation. Research shows that the hippocampus, a structure important for memory and learning, shrinks in persons who have been subjected to war-zone combat, child abuse, or other types of sexual abuse (Bremner, Randall, Scott et al, 1995). It has also been found that when a person is subjected to extreme stress, there is an excess of the neurotransmitter glutamate which decreases the brain’s capacity to inhibit sensory inputs (Gold, Goodwin, & Chrousos, 1991).
The early symptoms of sensory processing disorders in infancy are often related to regulatory problems, such as sleep difficulties, poor self-calming, very low or high activity level, atypical muscle tone with slowness in attaining motor milestones, and under- or overresponsiveness to sensory stimulation (DeGangi & Greenspan, 1988; DeGangi, 1991). Among infants with regulatory problems, hypersensitivities to touch, movement, visual, or auditory stimulation are prevalent (DeGangi & Greenspan, 1988). Infants with poor sensory processing often continue to persist in these problems, developing more serious developmental disorders by the preschool years if left untreated (DeGangi, Porges, Sickel, & Greenspan, 1993).
These problems can become lifelong, especially if the person never received treatment for their underlying problems of sensory integration. For example, Jules brought his young daughter for an evaluation because of her extreme social anxiety and aversions to touch, movement, and sound. As we talked about his daughter, Jules realized that he, too, suffered from the same constellation of symptoms since he was a young boy. He remembered his parents sending him to a psychiatrist as a child to treat his social anxiety, spending years “on the couch” but never being treated for his sensory problems. These severely impacted his motor skill development, relationships with others, and ease in navigating in the world, especially in feeling comfortable in various social settings. Jules felt enormously cheated out of an important opportunity for treatment. He stated, “It was like I had pneumonia and they denied me antibiotics to treat my illness. My whole life could have been so different.” As we worked with his daughter, we included Jules in the treatment. Although it was not as effective as it might have been if we had begun earlier in his life, Jules did feel some relief from his symptoms.
Infants and children experiencing distress from sensory input show their discomfort by grimacing, yawning, hiccoughing, averting their gaze, and a wish to flee. The child may become drowsy and sleep most of the time in an effort to “shut-down” the level of stimulation. Or the child may become hyperaroused and sleep fewer hours than expected for their age. Many children with sensory processing dysfunction are highly irritable, cry excessively, and have difficulties self-calming. For example, the child may be delayed in bringing their hand to mouth for sucking or in holding their hands in midline to self-calm. Some babies require intense vestibular stimulation (e.g., swinging, bouncing vigorously) to calm while others need more soothing types of movement experiences (i.e., slow rocking, riding in a car). Some infants can quiet if they suck on a pacifier or are swaddled tightly in a blanket, thus using the tactile sense to organize themselves. Similar problems may be seen in an older child. For example, Taylor could barely get through her school day without extreme agitation. A random touch on her back, other children bumping into her on the playground, or the noisy cafeteria where she ate lunch, all set her on edge. When she arrived home, the only thing that settled her was to listen to music with her headphones on while engaging in vigorous vestibular stimulation. This involved swinging outdoors on a swing, jumping on a trampoline, or rocking vigorously in a glider chair. Her parents found that they had to dim the lights to minimize visual and auditory stimulation. If she was prevented from doing these interventions for herself, her stress level would escalate profoundly. The end result would be a big fight with her younger brother, a huge tantrum over homework, and impulsive and erratic behavior.
Infants and children with developmental, learning, and emotional problems often experience constitutional problems related to the processing and integration of basic sensory information. In the field of temperament, the attribute of introversion has been linked to hypersensitivities. When there is a low sensory threshold and the person is easily overstimulated, they have difficulty synthesizing the range of sensory experiences (e.g., tactile, proprioceptive, vestibular, visual, or auditory inputs). This results in the child having difficulty in organizing purposeful actions in areas including communication, movement, and play. Often perceptual thinking and the regulation of affects are impaired as well.
The symptoms of toddlers with sensory integrative dysfunction occur in relation to how the child is developing autonomy, independence, and mastery of language and motor skills. The toddler with hypersensitivities usually displays discomfort by actively fleeing from the stimulus, retreating to a safe space, or by lashing out at the person or object that imposed the perceived “aversive” stimulus. Hitting, biting, and throwing are behaviors that may be related to hypersensitivities. Toddlers who display the range of sensory hyper- and hyposensitivities (i.e., sensory modulation problems) often show mood regulation problems. The toddler may quickly escalate from a content, happy mood to a full-blown temper tantrum, sometimes without warning or an attributable stimulus or event. Frustration tolerance is low and often the toddler with sensory integrative problems will become extremely upset when they are unable to problem solve how to manipulate or handle a particular toy.
The ability to self-calm often remains a problem for toddlers with sensory integrative dysfunction. Parents find that they must constantly give the child warning about changes in activity (e.g., going to a place, changing clothes, changing task). The toddler with these difficulties relies upon the parents to help them find ways to self-calm (e.g., holding a special toy in situations where impulse control is needed; constant verbal monitoring from parents). At the crux of the problem is the toddler’s difficulties problem solving and organizing a planned motor action in response to task or situational requirements.
Growing difficulties with separation often become apparent, particularly when the parent is the only person that provides a predictable sensory world for the child. Often the toddler with sensory integrative problems has problems playing in play groups, functioning in a day care situation, or other environments where the child is expected to play with peers and/or separate from a parent. Parents may find that they avoid busy environments, such as supermarkets, play groups, or shopping malls because their child becomes overwhelmed by the stimulation. Playing with peers is a challenge for the toddler with sensory integrative problems who may find the unpredictable touch and movement of other children very threatening. Some children react by becoming aggressive whereas others become avoidant and withdraw to safe places (e.g., under a table).
By the preschool years, delays often become apparent in fine and gross motor skills, balance, the planning and sequencing of motor actions, and coordination (DeGangi, Berk, & Larsen, 1980). Distractibility, sensitivities to touch and movement stimulation, language delays, and visual–spatial problems may be present (Ayres, 1979; Fisher, Murray, & Bundy, 1991). By the school-aged years, handwriting problems, dyslexia, attention deficits, and reading disabilities often emerge (DeQuiros & Schrager, 1979).
3. The concepts of sensory defensiveness and sensory dormancy
When children have sensory integrative dysfunction, they are apt to show fluctuations in their responses to sensory stimulation and may withdraw from the stimulation or may not seem to perceive the sensory input regardless of how intense or salient it may be. These two concepts of sensory defensiveness and sensory dormancy are important in understanding how children may respond to sensory input.
At one end of the continuum are children who show something called “sensory defensiveness.” These children are hypersensitive to sensory stimulation (e.g., olfactory, visual, tactile, auditory, movement) and are usually overly responsive to more than one sensory channel. At the other end of the continuum is the child who is the underresponder, a condition described as “sensory dormancy” (Knickerbocker, 1980; Kimball, 1993). When this occurs, there is too much inhibition of incoming sensory inputs; this results in a lack of sensory arousal. Typically the child with this problem will be passive and inactive with a failure to orient to important sensory stimuli. Fig. 9.1 depicts the continuum from sensory dormancy to sensory defensiveness.

Figure 9.1 Model of sensory registration.
Most individuals with sensory integrative dysfunction will either be hyperresponsive (e.g., sensory defensive) or hyporesponsive (e.g., sensory dormancy). Some children, however, have such severe sensory modulation problems that they fluctuate from one extreme to the other within the course of a short period of time. Normal variation is experienced over the course of the day as the individual responds to state of arousal, activity level, and sensory, cognitive, or motor demands of the task or situation. It has been speculated that sensory modulation problems underlie both sensory defensiveness and dormancy (Cermak, 1988; Kimball, 1993; Royeen, 1989; Miller & Lane, 2000). The concept of sensory defensiveness and dormancy is useful in considering the various types of sensory integrative dysfunction that are described in this chapter.
Some children with ADHD, hyperactivity, and sensory integrative problems are overstimulated, not only by the environment, but by their own behavior—squiriming in the chair, running, and movement. It becomes very difficult for them to organize purposeful tasks because they are struggling with overstimulation. However, for some children who appear to be overly active, they are seeking stimulation to increase their level of arousal. Because they do not have well-organized ways of doing this, they may appear hyperactive, aimless, or unfocused. It is important to determine what the child’s activity serves for him—to stimulate or calm.
In the following sections, common tactile and vestibular processing problems and motor planning difficulties of children with sensory integrative problems are described.
4. Clinical assessment of sensory integrative dysfunction
It is often useful to screen children for sensory integrative problems, therefore, a sensorimotor history questionnaire is provided at the end of this chapter. This checklist helps identify problems in the following areas: Self-regulation (activity level and attention); Processing of touch (sensitivity to touch and/or undersensitivity to touch); Processing of Movement (sensory seeking of movement and gravitational insecurity or fear of movement); Taste and Smell Sensitivities; Visual Sensitivities; Auditory Sensitivities; Social Skills; Motor Coordination and Posture; and Stress Management. Points are tallied and cutoff scores help determine if the child falls in the typical range, at risk, or deficit range. These scores can be useful in guiding treatment planning and intervention.
5. The tactile system
The somatosensory system is a primal sensory system which responds to various touch stimuli on the surface of the skin. It is a predominate sensory system at birth and remains critical throughout life as a major source of information for the central nervous system. An infant’s first movements are in response to tactile input, for example, when the baby is touched on the cheek, he will root toward the touch, trying to seek contact for sucking. Early learning depends upon making contact with the external world and is important in guiding experiences and interactions with the environment (Collier, 1985; Gottfried, 1984; Reite, 1984; Satz, Fletcher, Morris, & Taylor, 1984; Suomi, 1984).
The sense of touch involves the ability to receive and interpret sensation and stimuli through contact with the skin. Since exploration through the sense of touch is typically combined with limb movement, the tactile and proprioceptive systems have overlapping neural mapping (Kandel & Schwartz, 1981). Tactile receptors are activated by touch, pressure, pain, and temperature. The most sensitive parts of the body are the face, palms, soles of the feet, and the genitals. The least sensitive area of the body is the back. For example, if a person has an itch on their back, it may be hard to tell someone exactly where to scratch them but if the itch were on their hand, they could be very specific about it.
The tactile system has both a protective and discriminative system. The tactile protective system is activated by temperature changes of the skin, light touch, and general contact with the skin. Light touch, such as a tickle on the face, or a light stroke on the shoulder might cause someone to react with alarm if the touch occurred without them seeing it. Light touch acts as a protective mechanism to the central nervous system by giving warning if an outward stimulus is too close for safety.
In the newborn child, this protective reaction predominates until the baby becomes accustomed to being touched and learns to discriminate which tactile experiences are dangerous versus enjoyable. Through holding and cuddling, infants learn to become less sensitive to touching experiences. Swaddling an infant, that is, wrapping the baby tightly in a blanket is often necessary to help the infant remain calm and organized. Learning to tolerate these early touch experiences is one aspect of developing early self-regulation or homeostasis, that is, being able to take in sensory stimulation from the world and take pleasure from it.
The tactile protective system matures quickly and by the time the child has reached the preschool years; it no longer is a predominate sensory system. However, if the person is in a dangerous situation, their tactile protective system becomes activated along with other sensory responses, such as pupillary dilation. Children who are unable to tolerate light touch and are highly sensitive to tactile experiences, such as standing next to another child, wearing a long sleeved shirt, or even sitting on a chair surface are termed “tactually defensive.” If a person has sustained neglect or abuse, they are apt to show many symptoms of tactile defensiveness. Kimberly who had ADHD was roughly handled by her mother as a young child. She recalled incidents when she was held down by her mother to keep her still and to help her fall asleep. Her mother would wash her hair with such vigor, that as she grew into her teenage years, she couldn’t face away from the water faucet when she showered. She also remembered being tied in a chair by a teacher to keep her from running around the classroom.
A second important function of the tactile system is discrimination. The development of tactile discrimination is the ability to differentiate various textures, contours, and forms by feel. It plays an important role in initiation and planning of movement as well as exploration of the environment. Tactile discrimination is important for being able to localize where touch occurs on the body, to decipher if two or more points are being touched at the same time, to recognize shapes by feel, and to organize the body and its parts into an integrated scheme. Since hand skills involve many discreet manipulations of objects, fine motor skills are often compromised in the child with poor tactile discrimination (Haron & Henderson, 1985; Nathan, Smith, & Cook, 1986). It is touch combined with movement that allows for tactile discrimination to occur which is also an important aspect of motor planning.
When the tactile discriminative system is not functioning properly, the child often links a negative emotional meaning to touch. As a result, social interactions and emotion regulation are often maladaptive in children with poor tactile discrimination. For example, children learn to interpret different types of touch in social interactions, linking emotions to pleasant or aversive types of touch (e.g., aggression, love). The mother who burrows her face on her baby’s tummy in a game of touch should elicit smiling and laughter from her baby. The infant or child with poor tactile discrimination may avert gaze, pull away from the contact, or even cry. The toddler or preschooler may not tolerate close proximity with others and will respond by fleeing or engaging in aggressive actions.
In order for normal development to occur, this protective and discriminative system must be balanced. When the CNS malfunctions, as seen in learning disabilities and some emotional disorders, there is a tendency for the nervous system to regress to a developmentally earlier response which has greater survival value. In these children, the protective system is overaroused and they experience normally pleasant tactile stimulation as irritating or threatening. These behaviors have important implications for emotional development.
5.1. Tactile dysfunction
The tactile dysfunctions most commonly observed are tactile defensiveness and tactile hyposensitivities. Reactions to somatosensory stimuli can range from overresponsivity to underresponsivity. Overresponsiveness is more commonly characterized by feelings of discomfort and, typically, physical withdrawal from certain types of tactile stimuli. Ayres has described this as tactile defensiveness (Ayres, 1972, 1979, 1985).
Sensitivities to touch may be environmental (e.g., fleeing from contact of furniture; discomfort from clothing touching child), other-initiated (e.g., withdrawal from mother hugging child; avoidance of being in groups of children), or self-initiated (e.g., avoidance of touching textured objects). The child may respond aggressively by hitting or kicking, or by physically retreating (e.g., hiding under furniture). Emotional responses including hostility, aggressive behavior, and high irritability are not uncommon.
5.1.1. Tactile defensiveness
Tactile defensiveness is a severe sensitivity to being touched and usually involves an adverse reaction to initiating touch with non-noxious tactile stimulation. It has been suggested that the phenomenon of tactile defensiveness results from a failure of the central nervous system to modulate and inhibit incoming tactile stimuli (Fisher & Dunn, 1983). The child with tactile defensiveness will express feelings of discomfort and a desire to escape from the situation involving touch. The symptoms are much worse in situations where touch is induced on the child rather than when the touch is initiated by the child. The child responds by attempting to remove himself from the situation and will state, “I hate this game, it hurts” or “It tickles.” The child may pull away from being touched, run away from the adult, hit or kick aggressively, or hide under furniture. Even if the child is touched slightly, he may exclaim “Don’t push me!” or “Watch where you’re going!” Anxiety, discomfort, a need to withdraw, and hostility are common behavioral manifestations of tactile defensiveness.
The phenomenon of tactile defensiveness is characteristic of some children with learning disorders and has been correlated with hyperactivity and distractibility (Ayres, 1964; Bauer, 1977). It has also been documented in autistic children (Ayres & Tickle, 1980). Inadequate cortical inhibition of sensory processing and poor regulation in the reticular activating system has been speculated to cause symptoms of increased activity level, sleep–wake disturbances, tactile defensiveness, or withdrawal from sensory stimulation (Royeen, 1989). Table 9.1 presents common symptoms of tactile defensiveness.
Table 9.1
Symptoms of tactile defensiveness
Infancy:
• arching away when held (not high muscle tone),
• fisting of the hands to avoid contact of objects,
• curling of the toes,
• dislike cuddling,
• reject nipple and food textures (not oral-motor problem),
• strong preference for no clothing or tight swaddling,
• preference for upright or sitting position rather than lying on back or stomach,
• dislike face or hair being washed,
• hate car seat and other confining situations.
Toddler. Preschool and school-aged children:
• dislikes being touched or cuddled by others: pulls away from being held, cries or whines when touched, or hits back,
• distressed when people are near, even when they are not touching (i.e., standing nearby, sitting in a circle),
• avoids touching certain textures. Hates getting hands messy (i.e., finger paints, paste, sand, cooking or art),
• likes firm touch best and may enjoy games where there is very intense high contact (e.g., jumping into stack of pillows from a height, rock climbing, wrestling),
• prefers touch from familiar people,
• dislikes having face or hair washed. Especially dislikes having a haircut,
• prefers long sleeves and pants even in warm weather, or prefers as little clothing as possible, even when it’s cool,
• touches or handles objects frequently, needs fidgets in hands,
• bumps hard into other people or object,
• withdraws from being near others, particularly groups,
• may hit, kick, or bite others and is aggressive in play,
• has a strong preference for certain food textures (i.e., only firm and crunchy, or only soft),
• dislikes being dressed or undressed,
• bites or hits self; cutting, scratching or picking at skin,
• likes traction activities like hanging by arms or feet off of furniture or people,
• uses mouth to explore objects.
In this next part, two case examples are provided to highlight how tactile defensiveness may be observed.
5.2. Case description 1: tactile defensiveness in an autistic-like child
Andrew was a 5-year-old child with developmental delays and autistic-like tendencies. His developmental skills were developed to the 3–4 year level. Andrew’s underlying tactile defensiveness was considered to be his most predominant problem affecting his development. Behaviorally he exhibited a very short attention span and could only sit with a teacher-directed task for a few minutes at a time. When sitting in the chair, he constantly assumed bizarre positions and contorsions. Andrew engaged in many self-stimulatory behaviors including finger flapping, humming, and hanging and swinging on any apparatus that lent itself to this behavior.
Andrew would not permit others to touch him at all, including his family. If touched by another person, Andrew responded by pinching, biting, or kicking. At school, he was a severe behavior problem and would scream and kick when touched. Once these behaviors had occurred, Andrew could not be calmed for long periods of time. He often withdrew into places where he could avoid being touched, such as under a table or in a corner of the room, after which it would be very difficult to get him out of his hiding place. Andrew did not like other people to be too close to him and when in groups, Andrew would kick, bite, and scream. Tactile defensiveness was also observed in Andrew’s inability to tolerate having his face or hair washed. All of his clothing tags had to be cut out routinely. On one occasion, the tag was left in a new shirt by accident. Andrew began fidgeting with the tag, scratching his whole body. Over the course of the morning, he began to rip his clothing off and could not be controlled.
Andrew’s tactile problems are representative of a child with severe tactile defensiveness. Although Andrew’s problems are not solely attributable to his tactile disorder, it affected his capacity to develop appropriate interactional skills, attention, and self-calming. His severe tactile defensiveness needed to be addressed as a major component of his classroom and home management program.
Using guidance from the occupational therapist at school, Andrew’s parents found that his behaviors at home and school were much better when they instituted play times throughout the day that involved pleasurable contact with them. Before school, his mother rubbed lotion on his body using firm touch, emphasizing his palms and soles of his feet. Sometimes Andrew would use a surgical scrub brush and brush himself on his arms and legs while he and his mother sang songs together. His parents also found that if they gave Andrew some focused activity to do before school that involved heavy objects, it made a difference. Some examples of these activities included having Andrew helping them move chairs to the breakfast table or carrying his heavy back pack filled with a thermos, bean bags, and books on his back while he “checked” the house to see if all the lights had been turned off. After school they instituted a rough house play time with Andrew that involved deep pressure to his body. He particularly liked swinging on the tire swing outside and crashing his body into soft things like a large gymnastic ball that his mother would roll toward him. They thought of many creative interactive games using the concept of giving him heavy pressure to his joints and skin. For example, his mother and Andrew would kneel on opposite sides of a large foam “wall” and try to push the other person over. At the end of the day, Andrew needed time to settle himself down and responded well when his parents did soothing activities involving deep pressure. He loved lying back to back with his father while they sang songs and played with flashlights on the wall in the darkened bedroom. He also enjoyed sitting in a bean bag chair with his feet buried in a bin of dried beans or with a heavy quilt wrapped around his body while they read stories together.
5.3. Case description 2: tactile defensiveness in a child with motor and language delays
Michael was a 2-year-old with a moderate expressive language disorder and motor incoordination who was normal in all other areas of development. His parents were very concerned that he still had not regulated his sleep cycles. He had difficulty falling asleep and could only nap if driven around in the car. Bedtime was typically a major ordeal with many ritualized manipulative types of behaviors. The use of time-outs and behavioral procedures had not worked due to Michael’s strong fear of separation, being left alone, and his adverse reaction to being held. Calming techniques, such as swinging in a hammock didn’t seem to make a difference.
Michael was evaluated by an occupational therapist to determine if there were any sensory integrative problems underlying his sleep difficulties and motor incoordination. Throughout the testing, Michael was very fearful of being physically moved and touched by the examiner and, consequently, refused to attempt many tasks. An interview with the mother confirmed Michael’s hypersensitivities to touch and movement. He hated having his face washed and avoided messy activities, such as finger paints. He was very picky about the textures of clothing. In group situations, he tended to withdraw into hiding places (i.e., under a table or inside a tent) and became very irritable when in close quarters. He resisted being hugged and held, but would tolerate cheek to cheek contact with his mother on occasion. In addition, Michael avoided movement experiences, such as swings or slides and was very cautious about heights and climbing. He preferred to initiate movement activities rather than being moved by others. Sometimes he enjoyed making himself dizzy but became fearful if he moved too fast.
The treatment program was directed towards alleviating his tactile defensiveness and sensitivities to movement through activities that Michael could self-initiate. The tactile activities emphasized firm deep-pressure. He particularly enjoyed wedging himself between heavy mats, covering himself with pillows, and jumping into bins of plastic balls. Some of these activities were modified for use before bedtime to help Michael develop self-calming mechanisms.
5.4. Tactile hyposensitivities
Decreased tactile awareness or a hyporeactivity to touch is less often seen than tactile defensiveness. Children experiencing hyporeactivity to touch have decreased tactile awareness and do not experience touch unless the experience is very intense. Such a child may laugh and actually enjoy a firm pat on the buttocks when being disciplined. It is as if their thresholds for noticing or reacting to tactile stimuli are very high. Oftentimes these children do not seem to experience pain, are slow to initiate movement for tactile exploration, and therefore suffer from a type of sensory deprivation. It is common for these children to seek touch-pressure input. Some self-abusive behaviors may be interpreted as a means to trigger very high thresholds (e.g., biting self, head banging, cutting). Some children may bite themselves very hard, actually breaking skin without reacting. Another problem seen in children with diminished tactile awareness is that they are very slow in initiating movement and exploring objects by feel.
Very often the child with either tactile defensiveness or tactile hyporeactivity will exhibit a lag in motor development because of their inefficient use of touch in exploring objects. Frequently, children with tactile dysfunction have low muscle tone, contributing to poor sensory support for movement experiences. For instance, one may see the child sitting half on and half off a chair or sitting with the arm caught under their body with no apparent discomfort. It is important to note that the same child may exhibit both elements of tactile hyper and hyporeactivity to tactile experiences (e.g., crave deep pressure contact on hands but an aversion to light touch or certain textures on palms).
When an infant is underreactive to tactile input, they may appear very passive and content to be left alone. Often the baby does not cry during physically painful medical procedures. A low activity level is often observed. When these behaviors are observed, it is important to differentiate the child’s responses from other medical problems or a severe cognitive delay which can resemble these behaviors.
5.5. How tactile problems evolve over time
Because tactile perception is learned within the context of the social interactions (e.g., parent–child interactions), it is important to consider not only the infant’s tactile functioning, but what the caregiver and environment bring to the experience. Consider the effects of the tactually defensive parent on the infant’s emotional development. For example, the parent who is defensive to touch may avoid holding and cuddling their infant. Traumas early in life, such as child abuse or poor mother–infant bonding may affect the person’s responses throughout life in interactions involving touch. Likewise, the environment may cause a sensory deprivation, such as that experienced by the very premature infant who suffers a prolonged hospitalization with invasive medical procedures (e.g., oral intubation, heel sticks) and a minimum of holding and carrying from a loving caregiver. The effects of sensory deprivation are commonly seen in children who have been institutionalized in their early years.
Discomfort at tactile experiences becomes heightened as the child grows older and encounters more challenging and varied tactile experiences. For example, the child must accommodate to the touch of playmates and adults other than mom and dad’s familiar touch. Although the child’s own parents may have found ways to approach and touch their child in ways that feel acceptable to the child, other children and adults have not made this accommodation. As a result, the child’s tactile problems may appear worse.
As the child enters the second year of life, independence and mobility allow the child to flee from uncomfortable tactile experiences or to approach and touch those that are pleasurable. Some parents begin to notice that their child seems unusually active as they move from one unpleasant tactile experience to another. Some children are observed to mouth or bite toys, seeking hard deep pressure in an area of the body that can more easily adapt to incoming tactile sensations. The child often prefers intense deep pressure activities, such as rough housing with mom or dad.
Preschool and school-aged children with tactile hyper- or hyposensitivities often display fine motor difficulties because they lack the tactile discrimination to handle and manipulate objects within the palm and fingertips for refined use. Tasks, such as drawing with a pencil or buttoning are very difficult. The child may always look at their hands when they are manipulating objects. Mouthing of toys may still be present. There is often an avoidance of touching new textures with a preference for firm, hard toys. The child may have a strong preference for certain types of clothing, complain about clothing tags, and dislike having hair and face washed. More advanced tactile discriminative skills, such as stereognosis (i.e., detection of objects by feel alone) and graphesthesia (i.e., identification of letter or number drawn on a body part while vision is occluded) are usually delayed as well.
Play difficulties are common among children with tactile hypersensitivities. Destructive or aggressive play occurs frequently when the child is required to play with other children in close proximity. The child may touch other children with force even when trying to be gentle. If given a choice, some children withdraw from other children or find spaces to play that provide them with tactile security, such as a corner of the room.
5.6. Treatment approaches for children with somatosensory dysfunction
Below are some suggestions that may be useful in working with children with different kinds of tactile problems. If the difficulty is severe or complex, an occupational therapist should develop a treatment plan for the child and assure that the tactile input is integrating, not aversive (see Skill Sheet #2: Activities for problems of touch).
5.6.1. Techniques for the tactually defensive child
1. Provide opportunities in the environment that allow the child to self-initiate touch. Use enclosed areas, heavy objects, objects that vibrate, and materials that provide deep pressure on large body surfaces, such as a weighted blanket or a body pillow.
2. Encourage games with high contact with other people that allow the child to withdraw from other people in socially acceptable ways. Here are some ideas for interactive games that children usually enjoy. The children can play a game called “earthquake.” When lying under a stack of large foam blocks, the child keeps his body very quiet until signaled by the therapist to start the “earthquake” and knock the blocks over. In another version of this activity, the child lies very still on top of the blocks, then waits for the therapist to shake the blocks, causing the child to fall into the pile of blocks. The children can play inside a large stretchy tube, pulling in all directions as they move. Two children stand or kneel on each side of a large foam block and push hard, trying to knock over the wall. Or they can make a “people sandwich” with kids piling on top of one another while lying on a soft foam “cloud” mattress. Group games using a parachute or with a large stretchy tube do not provide direct physical contact between children but allow them safe physical boundaries that help them to tolerate being in close proximity with one another without touching.
3. Override the tactile system by using highly visual tasks. Putting stickers on body parts can be fun. Going inside an inflatable pup tent filled with plastic balls, playing dress-ups, or playing with small toys in a sand table are ways to incorporate the tactile and visual senses. Submerge the hands in a bin of dried beans or beautifully colored sand, making interesting designs in these mediums. The child can also work in clay or sculpey or do art projects with texture and color, such as working with tiles. In these activities, the emphasis should be on the visual channel versus the tactile stimulation. This can be done with the auditory system too. For example, taking a stick and pulling it over a grate to make a noise or holding a vibrating ball that makes humming noise are activities that emphasize the auditory over the tactile channel.
4. Use vestibular input coupled with the tactile stimulation for children who enjoy movement stimulation. For example, the child can ride prone in a hammock swing while “skiing” his hands in crazy foam on a wedge or he can bury his hands inside an inner tube filled with marbles and other small toys. Riding in a glider chair, sitting in a swing and kicking a heavy gymnastic ball with the feet, or lying prone in a hammock swing and pushing with the hands on the floor or against the wall to create the swinging movement are some other examples.
5. Scratchy textures, such as bristle blocks, sandpaper are often more accepting because they involve multiple points of contact and provide deeper input than smooth textures. Scrubbing the forearms, hands, back of the body, front of the legs and feet with a hand scrub brush may help desensitize the child. Sometimes this type of touch is more accepting because the brush provides multiple points of contact and deeper input than a smooth textured clothe.
6. The proprioceptive sense is very important in helping children to feel more comfortable with their tactile sensitivities. Resistive mediums, such as pulling theraputty, pulling a rubber hoop or heavy stretch doll, squeezing a “pop-it” man with the hands so his eyes, nose, and ears pop out, or burying the hands inside a bin of dried beans to find small objects are examples of how one may incorporate this into therapy. The adult should use firm, sustained contact when touching the child, providing input on the child’s back, abdomen, and pelvis first. Many children prefer a squeeze, release type of touch rather than a stroke or massage. When it is impossible to touch the child directly, it is often useful to begin with games like the “hot dog” whereby the child is wrapped up in a soft comforter, then the back is massaged with a large ball that rolls up and down the back in different ways (e.g., light tapping, firm rub) to provide “toppings” on the hot dog. The child may also lie under a heavy weighted blanket or sit with a weighted gel pad on his lap.
7. Address tactile defensiveness in everyday activities. For example, if the child avoids food textures, begin by using an electric toothbrush and Nuk toothbrushes on the gums and focusing on firm food textures first. Let the child self-initiate and provide touch to himself first if possible.
8. For the severely tactually defensive child, the therapist may need to set up a few things that are “done to” the child to help overcome the defensiveness (i.e., Pat Wilbarger’s brushing technique that involves rubbing the extremities, back, hands and feet with a surgical brush in a systematic way) (Wilbarger & Wilbarger, 1991). It is very important though not to suggest these types of activities to parents if there are significant problems in the parent–child relationship, if there might be potential abuse, or if the parent is already overly intrusive and controlling. In such instances, it is better for a therapist to initiate these adult-directed experiences.
9. Because of the intimate link between touch and emotions, it is critical that all tactile activities are introduced in a nurturing, caring way. The therapist should address the negative meanings that touch has become for both the child and parent. The parent who feels rejected by a noncuddly child; the child who interprets other children as hurting him when they are simply coming into his/her physical space are examples of these kinds of problems.
10. Encourage the family to keep a log of behaviors that occur after intervention including changes in sleep and attending behaviors. Tactile stimulation affects the nervous system at least 1.5 hour after administration. However, there is a loading effect and touch experiences occur all day long, so the therapist may not know when the peak effect has occurred. Watch for unusual behaviors, such as self-abuse, rapid breathing, sweating or flushing, destructiveness, problems sleeping, extreme restlessness. These behaviors are particularly hard to differentiate if the child has a motor problem and cannot move easily. If the child experiences negative effects from tactile stimulation, use slow rocking, firm pressure on the back and abdomen, and visual focus on a task (i.e., looking at a beautiful object). Taking a warm shower, wrapping tightly in a blanket, or putting an ice pack on the skin are other strategies to counteract a strong tactile defensive response.
5.6.2. Techniques for the child with hyporesponsitivity to touch
1. Registering touch is the central issue for children who are undersensitive to touch, therefore, the therapist needs to provide tactile experiences that force the child to attend to the fact that they are receiving touch. The stimulation needs to be done by combining touch with another sensory channel—vestibular, auditory, visual. It is also important to force an adaptive response from the child, thus giving them a motor action that goes with the tactile input. For example, one activity may be wrapping the child’s hand up in resistive putty, then waiting for child to look at his hand and figure out what to do about it. The therapist may wrap the child up in a large piece of paper to be a “hot dog” instead of using a blanket so that the noise of the paper orients the child to the touch.
2. Vibration and traction are helpful to introduce, thereby using proprioception as the main sensory channel. Cooking activities and carpentry that use electrical and vibrating tools are examples. Hanging from a chin-up bar, rock climbing, and resistive movement activities (i.e., elliptical machine, skiing) are very helpful.
3. If the child has self-abusive behaviors, institute a daily regime, several times per day whereby the therapist applies light touch and stroking to the areas that are affected (e.g., bit, hit, etc). If the child hits his head, be sure to provide input to both the face and hand. Make it a routine that is fun that the child can anticipate. Warm scented lotion can be used or a loofah sponge to provide the input.
4. Remember: The child who is underreactive to touch almost always has elements of tactile defensiveness!
6. The vestibular and proprioceptive systems
Like the tactile system, the vestibular system develops early, enabling the fetus and infant to receive and respond to specific movement stimuli. In utero, the fetus receives constant vestibular stimulation from movement of the amniotic fluid as well as the mother’s own body movements. Because of its role in assisting the infant in orienting himself in space and in initiating exploratory and adaptive movements, the vestibular system, along with the tactile system, is particularly critical for development of basic functions in the young infant. The vestibular system has an impact on the development of body posture, muscle tone, ocular-motor control, reflex integration, and equilibrium reactions (Keshner & Cohen, 1989). These vestibular-based functions have a strong impact on the development of motor skills, visual–spatial and language abilities, hand dominance, and motor planning (Ayres, 1972; Clark, 1985). It is important for coordination and motor planning of the two body sides. In addition, the vestibular system plays a role in arousal and alertness. This is why visual alertness and attention increase when the person is moving.
Another important function of the vestibular system is to provide gravitational security when moving in space. A secure sense of where the body is in space contributes to the development of emotional stability. A child who lacks adequate vestibular functioning may be insecure in his body movements, fearful of movement in space particularly when the feet leave the ground, and is likely to exhibit emotional insecurity. Fear of heights is common to this problem and a fear of trying new and challenging movements (i.e., rock climbing, roller skating, or skiing).
The proprioceptive system develops through weight bearing and movement against gravity. This sense is critical in the maturation of reflexes, particularly the equilibrium or balance reactions, in perception of body position and movement in space, and in providing security and stability as the child moves. Visual feedback is important in developing proprioception because it helps the person to monitor their posture and movement. The proprioceptive sense develops in conjunction with the tactile and vestibular senses.
The primary purposes of the vestibular system are summarized in Table 9.2.
Table 9.2
Primary purposes of the vestibular system
1. Detect motion of the body
2. Detect and respond to the earth’s gravitational pull
3. Detect motion within the visual field
4. Influence muscle tone and posture
5. Influence motor coordination including bilateral motor control and sequencing
6. Impact body scheme
7. Provide gravitational security during body movement especially when challenged by heights or uneven surfaces
8. Modulate arousal and alertness for attention and calming
9. Provide visual efficiency skills (smooth visual tracking, eye convergence, binocularity, and coordination of hand and eye movements)
6.1. Vestibular-based problems
Because the vestibular system is very complex in its anatomy and neurophysiology, there are many types of vestibular-based problems (Fisher et al., 1991; Kimball, 1993). The most common vestibular-based disorders are presented in Table 9.3.
Table 9.3
Common vestibular-based disorders
• Gravitational insecurity (e.g., fear of moving the body in space)
• Underresponsiveness to movement in space (e.g., don’t perceive movement)
• Intolerance or aversive response to movement
• Postural-ocular movement disorder (e.g., eyes don’t coordinate well with body movements)
• Vestibular-postural deficits (e.g., low muscle tone, poor balance and posture)
• Bilateral integration and sequencing problems (e.g., difficulty with two-sides of body coordinating in sequenced movements like skipping)
• Motor planning problems associated with the underlying vestibular disorder
Infants with vestibular hypersensitivities typically show an intolerance for low-to-ground positions (e.g., prone or supine), a strong preference for upright postures, low muscle tone, slowness in developing motor skills, delayed balance, and/or fear of irregular or unexpected movement (DeGangi & Greenspan, 1988). When the infant is underresponsive to movement in space, the infant seems to crave movement and may become very fussy and demanding unless the parents provide movement stimulation for them. Once the baby is more adept at moving about, he or she may rock vigorously while sitting or on hands-and-knees. The infant may seek swinging for long periods of time and particularly enjoy rough housing with parents.
Vestibular processing problems in the child may take the form of hyper- or hyposensitivities to movement. When the child is gravitationally insecure—that is, fearful of movement experiences with a strong preference for movement activities near to the ground, there is often an accompanying separation anxiety disorder. The child relies heavily upon the parent to provide safety in new situations, such as helping them to find a place to play where other children won’t bump into them, causing them to fall. Since the child with gravitational insecurity usually dislikes playing on playground equipment, one usually sees the child with this problem standing close by an adult when outside or preferring to play with small manipulative toys. The child’s play in large space is very constricted, playing in a small area, even when engaged in play with cars and trucks on the floor.
When a toddler is underreactive to movement stimulation, different issues emerge. Toddlers are notorious for their desire to test limits and attempt activities that allow them to master new motor skills. The child who is underreactive to movement often challenges parents by climbing onto dangerous surfaces, jumping from unsafe heights, or trying a movement activity that exceeds their motor capacity, such as climbing high on a jungle gym. Often the child who is underreactive to movement is fearless and constantly tests limits. They may crave movement activities and become very upset when restrained from continuing to swing, climb, or spin. Parents often report that on days where the child is unable to engage in such movement activities, the child becomes very irritable, tantrums frequently, and has difficulty with sleep.
In addition to gravitational insecurity and vestibular hyporeactivity, the preschool and school-aged child with vestibular problems often has problems in postural control, balance, and sequencing and coordination of movement. The child may have poor equilibrium reactions in different body positions. When sitting at a desk, the child may be fidgety with extraneous body movements due to weak trunk stability. When asked to engage in activities, such as walking on hands in a wheelbarrow walk or climbing a trapeze bar, the child may show weakness of the trunk and neck. As a result of weakness at the shoulders, the child may have poor distal prehension, holding small objects with the pads of the fingers rather than the fingertips. It is not unusual for the child to have ocular-motor problems as well, such as difficulties looking up from their paper to the chalkboard and back again to their paper.
Vestibular dysfunction is often observed in combination with bilateral integration problems, particularly in children who have postural deficits. Bilateral motor integration involves the ability to coordinate the two body sides and develop lateralization (Magalhaes, Koomar, & Cermak, 1989). Children with problems in this area frequently do not establish a hand dominance by school-age. Frequently the child will interchange hands with no consistent preference for one hand. Bilateral assistive skills where one hand acts as a specialized hand and the other as an effective stabilizer are difficult. For example, simple tasks, such as buttoning and scissor cutting are delayed. Reciprocal bilateral movements, such as skipping, jumping, or alternating the hands in a drumming pattern are difficult. Oftentimes the child lacks precision in hand function and cannot sequence hand movements. The child may lack symmetry and control in large body movements. As a result, the child is often very clumsy and stiff in gross motor tasks, such as rolling and walking since these movements require coordination of the two body sides. The child lacks flexibility in rotating the trunk, and there is also a strong resistance in crossing the body midline. Consequently, the child may turn the entire body when required to cross the midline rather than rotating the trunk. Table 9.4 presents many of the traits of children with vestibular problems.
Table 9.4
Symptoms of vestibular hyper or hyposensensitivities
Vestibular Hypersensitivities:
1. Easily overwhelmed by movement (i.e., car sick).
2. Strong fear of falling and of heights.
3. Does not enjoy playground equipment, amusement park rides, and avoids rough housing and active sports or movement activities.
4. Is anxious when feet leave ground.
5. Dislikes having head upside down.
6. Slow in learning skills, such as climbing up stairs or playground equipment and relies on railing longer than other children same age.
7. Enjoys movement which she/he initiates but does not like to be moved by others, particularly if the movement is unexpected.
8. Dislikes trying new movement activities or has difficulty learning them.
9. May have a history of being delayed in skills like walking.
10. Feels anxious and perhaps panicky in stressful movement situations.
Under-responsiveness to movement:
1. Craves movement and does not feel dizziness when other children do.
2. Likes to climb to high, precarious places. No sense of limits or controls.
3. Is in constant movement, rocking or running about or is fidgety and restless.
4. Likes to swing very high and/or for long periods of time or daredevil amusement park rides.
5. Frequently rides on the merry-go-round while others run around to keep the platform turning.
6. Enjoys getting into an upside-down position.
In this next section, details about the different types of movement disorders are described.
6.2. Gravitational insecurity and intolerance for movement
Postural or gravitational security seems to play an important role in the development of emotional stability as well as balance, postural mechanisms, and spatial perception (Fisher & Bundy, 1989; Matthews, 1988). Children who are hypersensitive to movement are usually overwhelmed by intense movement stimuli, such as spinning, frequent changes in direction and speed, or unusual body positions (e.g., inverted). Typically they are fearful about leaving the earth’s surface and are thus called gravitationally insecure (Ayres, 1979). Often they display considerable autonomic responses (dizziness, nausea) during and after any type of vestibular stimulation. Increased sensitivity to vestibular stimulation can result in motion sickness (Baloh & Honrubia, 1979).
The gravitationally insecure child demonstrates an extreme fearfulness of moving in space. Children with gravitational insecurity typically have a strong preference for upright positions, avoid rotational movement patterns, such as rolling, prefer close-to-ground positions (i.e., W-sitting posture), “lock” the body and neck in rigid postures to avoid movement stimulation, and tend to avoid movement activities. Not only are they fearful of body movement in space, but they resist any change in their body which they may perceive as threatening. Movement that is imposed is particularly upsetting to the child. The emotional response that accompanies gravitational insecurity is associated with a sudden change of head position, a displacement in the body’s center of gravity, or the feet suddenly leaving the ground. As a result of insecurities in moving in space, children with gravitational insecurity tend to be emotionally insecure also. They frequently display fearfulness of new situations, rigidity, and a resistance to change. It has been hypothesized that gravitational insecurity may be due to poor modulation of otolithic inputs (Fisher & Bundy, 1989). In infants one may observe a strong preference for sameness in routines with crying and agitated behavior when routines vary, a strong need to be held and carried constantly, and a fearfulness of certain body positions (e.g., back or stomach). Some individuals experience an intolerance for movement and experience considerable autonomic discomfort during movement activities. The child may also exhibit gravitational insecurity as well. Typically the child feels nauseated and dizzy, particularly during rapid movement activities, such as spinning. It is not infrequent for such an individual to experience motion sickness in a car or boat ride. It is hypothesized that the individual with intolerance for movement is hyperresponsive to semicircular canal stimulation (e.g., spinning) (Fisher & Bundy, 1989). Since gastrointestinal symptoms are common, vestibular-vagal connections are also involved. Sometimes a person with intolerance for movement has visual motion sensitivity and feels autonomic responses while watching spinning or swinging objects, or watching motion pictures that assimilate movement or flight in space (Fisher et al., 1986).
6.3. Hyporeactivity to movement in space
When children have a high tolerance for vestibular input (hyporeactivity to movement), the behavioral repertoire is different. These children may seek movement experiences and yet do not seem to profit from them. One may see explosive movement quality, poor judgment in starting and stopping movement activities, or difficulty with transitional movements. Children with vestibular problems typically exhibit low muscle tone and may not be able to move against gravity easily enough to stimulate the vestibular system in a variety of movement planes. As a result, poverty of movement provides fewer opportunities for developing vestibular output for postural control and balance. Children who are hyporeactive to movement usually crave movement and do not display any evidence of autonomic responses, such as dizziness associated with spinning.
6.4. Vestibular-postural deficits
Vestibular-postural problems are among the most common type of vestibular-based deficits. Frequently children with minor neurological impairments have difficulty with postural reactions including balance, ocular-motor control, and visual–spatial skills (Steinberg & Rendle-Short, 1977). Children with severe emotional and behavioral problems have also been reported to display deficient equilibrium and postural responses, decreased postrotary nystagmus, and an absence of autonomic responses, such as dizziness and nausea following vestibular stimulation (Ottenbacher, 1982).
The primary problem underlying a vestibular-postural problem is inadequate postural control. The neck and trunk muscles provide stability in movement, and their development provides the foundation for postural control. If the proximal musculature is not well developed, the child is often unstable in maintaining body postures, has poor balance, and may have poor fine manipulation and locomotor skills.
6.5. Treatment approaches to address vestibular problems in children
6.5.1. General treatment principles
In treating children with vestibular-based problems, therapy needs to be directed toward normalizing the child’s responses to sensory input and in developing more adaptive and functional motor skills. Since many children with vestibular dysfunction also exhibit emotional problems, these need to be addressed in the therapeutic process. The major principle underlying treatment of vestibular problems is the importance of improving the child’s ability to organize and process vestibular input provided during meaningful events, thus allowing the child to produce an adaptive response to the environment. The child’s ability to actively control the sensory stimulation while simultaneously engaging in purposeful motor activity is essential to the intervention process.
Sensory integrative therapy utilizes vestibular stimulation to influence balance, muscle tone, oculomotor responses, movements against gravity, postural adjustments, and activity level. Linear movement activities (e.g., walking, jumping) assist the child to acclimate in relation to the environment, facilitating the development of an understanding of the body position and body movement in space while rotary and irregular movement activities (e.g., spinning, accelerating and decelerating, playing in unusual positions) provide powerful input to the system for arousal and alerting. A major premise of sensory integrative therapy is that movement activities should be self-initiated to elicit adaptive responses. Since children with severe tonal disturbances often have considerable difficulty self-initiating adaptive movement, opportunities for active, purposeful movement need to be provided via mobile surfaces (i.e., water beds, large foam mattress “clouds”).
There is no set prescription for therapy for a child with vestibular dysfunction. Since each child brings with him a unique combination of characteristics, these must be addressed in the therapy process. Therapeutic activity should involve the child’s choice of activity guided by his or her own interest and skill. Play is the medium through which therapy is adapted. For example, the child may develop an imaginary game where he is flying through space like “Flight Man.” The therapist seeks to structure the environment to facilitate the child’s responses. Table 9.5 presents a list of guidelines when providing vestibular stimulation activities.
Table 9.5
Guidelines for vestibular stimulation activities
1. The child should always be actively involved in the movement versus imposing the movement on the child, (e.g., pushing himself on equipment, or actively involved by telling the therapist when to stop or start the motion).
2. Vestibular stimulation should always be provided within the context of what the child is needing to work on, that is, improved postural control, bilateral integration, or better attention and self-calming.
3. Without a purpose, vestibular stimulation can be extremely disorganizing.
4. Activities should be selected that provide both ocular and auditory inputs since the vestibular system works optimally in conjunction with visual input from the eyes, auditory cues from the environment coupled with proprioceptive input to the joints. The Astronaut Training program is an example of this type of treatment, (e.g., the lights may be dimmed while the child navigates through a tunnel on a scooter board with his flashlight) (Kawar, Frick, & Frick, 2005).
5. Proprioceptive input may be enhanced through the use of weighted objects, firm pressure to joints, movement against gravity (i.e., pushing a scooter board up a ramp), traction, or resistive activities (i.e., kneading bread, working with heavy tools).
6. In order for responses to vestibular stimulation to be adaptive, the movement should be provided in all planes and in all directions of movement (e.g., the type of movement should be varied—head to toe rocking, side to side, forward-back, or rotary movements (orbital or circular spinning). Vestibular input may vary in terms of speed, direction, regularity and timing, and plane of movement).
7. Low frequency sounds have a direct calming influence on the vestibular system, therefore, the client may benefit from auditory interventions provided by an occupational therapist that employ bone conduction of sound stimulation (www.integratedlisteningsystems.com; www.advancedbraintechnologies.com).
As with any sensory stimulation, the child’s responses should be watched carefully to assure that it is perceived as pleasurable and useful to the child as they learn new skills. Autonomic responses, such as increased respiration, flushing or pallor, sweating, nausea or yawning, or severe dizziness and loss of balance should be observed. They may not always occur immediately during or after the stimulation. Instead the child may become disorganized or ill later in the day or after additional vestibular stimulation (i.e., ride home) loads the system to its maximum toleration level. Slow rocking with firm pressure on the abdomen, use of firm tactile input, and cognitive games, such as counting or singing will help the child to regroup if the input has been too intense.
6.5.2. Approaches for hyperresponsivity to movement
Very different treatment approaches are used with children who are under- versus overresponsive to movement stimulation. The child with gravitational insecurity needs a slow, gradual approach to introducing movement. This child responds best when movement is linear, such as forward-back or side-to-side since gravitational insecurity is hypothesized to be the result of poor modulation of otolithic input. The reason that this type of input is so calming and easy to accept is that it does not involve any rotary movements or large movement displacements of the head in space. Orbital spinning (modified spinning with face remaining in one direction) is usually accepted as well. Coupling movement activities with firm deep-pressure activities (i.e., holding a pillow on the lap or draping a weighted blanket on the lap or shoulders, or lying prone on a gymnastic ball) help the child to organize the movement experience through the sense of touch. The child needs a very gradual approach, starting with activities that are close to the ground. In individuals who are highly resistant to even the slightest bit of movement often do better with auditory integration activities (e.g., bone conduction therapy that stimulates the vestibular system via the auditory channel).
If vestibular stimulation is imposed or forced on the child, it can be more disorganizing than integrating. Therapy must be carefully graded to challenge the child, yet within the confines of what the child can tolerate and integrate. The child should be moved slowly and in a rhythmical movement. Maintaining close body contact with the child helps him to learn to tolerate any movement, thus providing inhibition through the tactile sense. By helping the child to anticipate where his body is moving in space by providing visual or auditory cues also helps to know where he is about to move. Activities should be selected that are first close to the ground (i.e., a sit ’n spin or T-stool). The child may need to be enticed to just touch moving equipment or to put a favorite toy on the swing in the first weeks of treatment. In this way, the child may gradually learn to tolerate the visual component of watching the movement before he is expected to move in space. If the child is allowed to decide upon a movement and then enact the movement, it helps to modulate the vestibular input.
6.5.3. Techniques for hyporeactive responses to movement in space
The child who is hyporeactive to movement in space often craves spinning and will seek fast moving, rough kinds of games. This type of child may disorganize very rapidly and without warning and is often reckless and impulsive. Vestibular stimulation needs to be carefully directed and combined with purposeful, goal-directed activities so that the child learns to control the sensory stimulation and keep his activity purposeful and organized. Movement stimulation activities that are very intense and stimulating should be coupled with inhibitory or calming ones. Rotary (circular spinning, rolling down a ramp) and irregular, fast moving input which require the eyes to constantly adapt to a new visual focus are typically used in treatment for this type of child. Inverted body positions (upside down) are also highly stimulating because they involve a complete displacement of the head.
6.5.4. Techniques for vestibular-postural problems
Intervention directed toward improving postural mechanisms should focus on improving muscle tone, developing antigravity postural control, improving muscle cocontraction, and developing righting and equilibrium reactions. Intervention should first be directed towards improving muscle tone and developing antigravity postural control. Through the use of basic anti-gravity postures combined with vestibular stimulation and functional activities, muscle tone may be improved. Sometimes specialized handling techniques may be required to increase tone in the low tone child. For example, one may have the child sit on inflatable equipment to work their postural tone and balance. A variety of materials, such as stretchy ropes, resistive therapy bands, or heavy weighted toys help to stimulate tone as well.
6.5.5. Approaches for inattention and problems with self-calming
Vestibular stimulation is very powerful as a tool to help regulate arousal levels to enable self-calming and focused attention. One of the strategies to decrease a hyperaroused state in a child is to use sensory inhibition to diminish arousal prior to bedtime or at other times when the child is overly active and needs to sit quietly for learning or table top activities. Linear movement activities (e.g., forward-back and head-to-toe rocking, swinging coupled with low frequency sounds) are calming and serve to inhibit the reticular activating system via the vestibular system. When the child is unable to fall asleep on his own, movement may be introduced to dampen hyperarousal. Crib cradles (e.g., a hammock swing designed for the crib), a vibrating mattress, or a water bed mattress help to further soothe the overaroused child. Swinging the child within a soft blanket filled with pillows or lying with the head inverted slightly may also inhibit arousal level (see Skill Sheet #3: Moving for Mood Regulation and Sleep).
7. Sound sensitivities
A very common and often overlooked problem is auditory hypersensitivities. These are more difficult to diagnose because sounds have a loading effect on the nervous system. We are constantly subjected to traffic noises, sounds of appliances, screaming children, or other random noises. Children with sound sensitivities often have troubles with auditory figure-ground (e.g., listening to a conversation in a busy restaurant when hearing is not a problem) and will feel stressed and overwhelmed by how taxing listening in noisy places is on them. Auditory integration activities are often helpful in reducing these types of auditory hypersensitivities (www.integratedlisteningsystems.com).
8. Motor planning disorders
Developmental dyspraxia, also known as a motor planning disorder, is a sensory processing deficit which is often related to tactile and/or vestibular processing disorders. The problem lies not so much in the processing of sensory input or the ability to produce the movement skill, but in the intermediary process of planning the movement. The child with developmental dyspraxia has significant problems in planning and directing goal-directed movement, skilled, or nonhabitual motor tasks. Because the dyspraxic child lacks internal cognitive organization to focus thoughts and actions, the child is often vulnerable to distraction (Ayres et al., 1987). The distinct types of motor planning problems are presented in Table 9.6. Children with vestibular or tactile dysfunction may exhibit any of these types of dyspraxia (Ayres, 1985; Conrad, Cermak, & Drake, 1983; Cermak, 1985).
Table 9.6
Types of motor planning problems
| Postural dyspraxia | Inability to plan and imitate large body movements and meaningless postures. |
| Sequencing dyspraxia | Difficulty making transitions from one motor action to another and in sequencing movements (e.g., thumb–finger sequencing). |
| Oral and verbal dyspraxia | Inability to produce oral movements on verbal command or in imitation, a skill that affects speech articulation. |
| Constructional dyspraxia | Inability to create and assemble three-dimensional structures (e.g., block bridge). |
| Graphic dyspraxia | Inability to plan and execute drawings. |
| Dyspraxia involving symbolic use of objects | Inability to use objects symbolically. |
The underlying problem in developmental dyspraxia is the ability to organize a purposeful plan of action. The components that are needed include:
1. Stage 1: Ideation: In this first stage of motor planning, the child must develop the conceptual organization of the skill or task. The child needs to link the feeling of enacting the motion or action with the concept of which actions lead to task completion. In treatment, the occupational therapist may move the child through the action while describing what is happening. Sometimes children are more interested to try a difficult task if they have experienced what it feels like to move through the motions. Once the child has engaged in the task successfully a few times, it is important to then vary the task demands slightly to present a new challenge. In this way, the child learns to self-correct and to execute new movement patterns.
2. Stage 2: Planning the action: Before the child can plan out what he wants to do, he must be prepared to act. He needs to be motivated to do the action, therefore, it is important to find activities that excite the child and solicit his interest and involvement. The first step in learning to plan an action is to be able to experience it and to verbalize or conceptualize what needs to happen. Once the child has enacted the action with a model or the therapist’s assistance, he needs to understand what the end goal will be and how to get there. Selecting activities that give sensory feedback throughout the sequence helps the child to construct a plan. For example, if an obstacle course is used, the child may crawl through an opening in a large foam tunnel, then pull himself on the scooter board by holding a resistive rope, and lastly, swing while pushing over the large sandbag man. Each of these would have distinctly different sensory inputs that would help him mark each event in time and space.
3. Stage 3: Executing the plan: This is often the easiest stage of praxis. An important component of plan execution is self-correction and verbal mediation. The therapist may help the child to articulate what he is doing to help him link language with motor actions. Verbal commands from the therapist while the child engages in a task help to organize the sequence for the child. Once the child has consolidated his actions with verbal guidance from the therapist, he should then be helped to articulate what he is going to do next.
The most common types of motor planning disorders observed in children with somatosensory and vestibular-based problems are related to postural, sequencing, bilateral motor coordination, constructional, and praxis to verbal commands (Ayres, 1985). An emphasis of therapy is on the ability to plan whole body movements in space and to combine the body with objects. Through the use of postural patterns of flexion and extension against gravity, trunk rotation, and diagonal rotary patterns, the child can learn to map simple body movements in space. These postural patterns are combined with functional activities so that the movement pattern has a purpose for the child. Therapy focuses on the use of sensory stimulation in combination with a strong visual component to help the child to see what he is doing in space and to visualize the effect his actions have on objects. For example, by having the child sit in a hammock and swing to kick over a tower of cardboard blocks will give him vestibular, proprioceptive, and visual feedback to consolidate the motor plan of kicking over the tower. The major emphasis is therefore placed on relating the body in space in relation to objects.
By the second year of life, motor control and motor planning problems begin to become more evident. In the area of motor control, one observes the child having difficulty coordinating use of the two hands in simple bilateral tasks, such as putting together pop beads. Muscle tone may be diminished. For instance, the child may sit or stand in a slumped body posture. Balance may also be poor with problems in learning tasks, such as descending steps while holding a railing.
Motor planning problems become evident as the child experiences extreme frustration over tasks that he cannot problem solve. Because of the motor planning disorder, the child often breaks toys easily, then becomes very upset when he cannot fix them. Often the child relies heavily upon the parents to guide them whenever an activity is going to change. Some parents find that they need to prepare their child several days in advance about upcoming events to prevent major emotional upsets. The parents often explain everything that is going to happen as well as giving verbal feedback while the activity is occurring. The child seems to struggle with getting started and carrying out the necessary steps to complete the task. Activities with sequences, such as undressing and dressing are struggles for the child.
Some of the common symptoms of the child with dyspraxia are delays in dressing and in fine and gross motor skills involving imitation, sequenced movements (i.e., lacing, skipping), and construction (i.e., building from a block model). Poor accuracy of movement is observed and skilled hand movements, such as handwriting are very difficult for the dyspraxic child. Their movement quality may be explosive with poor judgment of force, speed, and aim. Speech articulation may be poor since this is also a planned, skilled motor activity. Nonhabitual tasks are very difficult for the dyspraxic child, therefore, they prefer routines and strongly resist changes. Transitions from one activity to the next may cause behavioral upset.
Initiation of new movement sequences or new organized plans of behavior are difficult. For instance, the child may not be able to tell you what he plans to do because he lacks an internal plan. As a result, one may see the dyspraxic child as becoming either very disruptive and aggressive, particularly when there is no external structure to organize the child, or the child may become very passive and prefer repetition of certain favorite activities, resisting new and different tasks. One may observe tantrums, aggressive behavior, poor play skills with peers, frustration, and a strong resistance to change. Some children become very controlling and manipulative because of their inability to control and impact their environment. Needless to say, poor self-concept is a major problem of the dyspraxic child. Tables 9.7 and 9.8 list some of the common symptoms of motor control and motor planning problems observed in children.
Table 9.7
Motor control problems in the child
1. Frequently breaks toys—cannot seem to judge how hard or soft to press when handling toys.
2. Trips over obstacles or bumps into them.
3. Falls frequently (after 18 months).
4. Slumped body posture when sitting or standing.
5. Leans head on hand or arm.
6. Prefers to lie down than sit, or to sit rather than stand.
7. Has a loose grip on objects, such as a pencil, scissors, or spoon.
OR grip is too tight on objects.
8. Fatigues easily during physical activities.
9. Is loose jointed and floppy; may sit with legs in a W.
10. Has difficulty manipulating small objects, particularly fasteners.
11. Eats in a sloppy manner.
12. Does not use two hands for tasks that require two hands, such as holding down the paper while drawing, holding the cup while pouring.
Table 9.8
Motor planning problems in the child
1. Fear of trying new motor activities. Likes things to be the same and predictable (i.e., routines).
2. Difficulty making transitions from one activity to next.
3. Must be prepared in advance several times before change is introduced.
4. Cannot plan sequences in activities, needing structure from an adult.
5. Easily frustrated.
6. Is very controlling of activities.
7. Difficulty playing with peers.
8. Aggressive or destructive in play.
9. Temper tantrum easily.
10. Did not crawl before starting to walk.
11. Difficulty with dressing and sequenced motor actions
8.1. Treatment of developmental dyspraxia
There are three primary processes that must occur in treatment for the child with developmental dyspraxia. These include:
1. developing the conceptual organization of the skill or task;
2. developing a plan or program of action; and
3. executing the plan.
It is rare for a child to have a motor planning problem without difficulty in the tactile or vestibular system. Treatment for children with vestibular-based motor planning problems should first focus on vestibular awareness, therefore, vestibular stimulation activities should precede motor planning tasks in a therapy session. Postural and other motor problems associated with the vestibular-based motor planning problem should be addressed in the treatment process as well.
Step 1: Ideation: In this first stage of motor planning, the child with vestibular-based dyspraxia will have difficulty initiating purposeful movement. The child needs to link the feeling of enacting the motion or action with the concept of what actions lead to task completion. The therapist may move the child through the action while describing what is happening. By using vestibular stimulation in a very specific way, the child can attach meanings to the action. For example, a child may not be able to motor plan how to push himself on a scooter board. The therapist may hold the child’s hands and contrast fast and slow movement on a scooter board in a game, then vary other task characteristics, such as holding a hoop versus the therapist’s hands, or riding down a ramp or inside a tunnel. Each of these variations of the same action will help the child to conceptualize the motor action that is required to propel through space on the scooter board. Motor planning activities should be varied according to sequence, ordering, position, and timing.
The child may not be able to choose a motor task at first because he does not have a concept of what he is able to do with the different toys and materials. The therapist may select a simple planning task, and then model how to do it. For example, the therapist may demonstrate jumping off a platform into a large bin of balls, a task that offers both challenge and success. If the child shows fear or is unable to complete the action required, the task should be modified to assure that the child can succeed. Sometimes children are more interested to try a difficult task if they have experienced moving through the motions. Once the child has engaged in the task successfully a few times, it is important to then vary the task demands slightly to present a new challenge. In this way, the child must learn to self-correct himself and to execute new movement patterns.
Step 2: Planning the action: Before the child can plan out what he wants to do, he must be prepared to act. He needs to be motivated to do the action, therefore, it is important to find activities that excite the child and solicit his interest and involvement. The first step in learning to plan an action is to be able to experience it and to verbalize or conceptualize what needs to happen. Once the child has enacted the action with a model or the therapist’s assistance, he needs to understand what the end goal will be and how to get there. Selecting activities that give sensory feedback throughout the sequence helps the child to construct a plan. For example, if an obstacle course is used, the child may crawl through an opening in a large foam tunnel, then pull himself on the scooter board by holding a resistive rope, and lastly, swing while pushing over the large sandbag man. Each of these would have distinctly different sensory inputs that would help him mark each event in time and space.
Verbal mediation is an important aspect of learning to motor plan. The therapist may help the child to articulate what he is doing to help him link language with motor actions. Verbal commands from the therapist while the child engages in a sequenced task help to organize the sequence for the child. Once the child has consolidated his actions with verbal guidance from the therapist, he should then be helped to articulate what he is going to do next.
9. Case description: the gravitationally insecure child with developmental dyspraxia
Emily was a 4.5-year-old who lived in constant fear and panic whenever she had to move, get on playground equipment, or learn a new motor skill. She spent most of her time either glued to her mother’s side, usually wanting to be picked up and carried, or clinging to her teacher at school. She had very low muscle tone and sat at the table with her trunk collapsed and her shoulders in a tense, elevated position. Her delay in motor skills and motor planning problems coincided with problems with balance. She frequently fell and as a result, her body was covered with bruises.
Emily was a very shy and withdrawn child and her movement sensitivities caused her to back away from entering play with other children. If Emily was presented with a motor task to do like participate in an obstacle course at school, Emily would cry silently even when the activity was very appealing.
Formal testing of Emily’s sensorimotor problems showed that she was very weak in postural control, collapsing to the floor in positions like a wheelbarrow walk. She sat in a W-sitting posture, and her body seemed to drape on furniture or she would lie on the floor. Emily always seemed out of energy, yawning constantly, and complaining that she was “too tired” to do anything requiring effort. If we could get her to run or move in any way, it was notable how stiff and awkward she looked, with very slow and deliberate movements as if she had to think “right foot, now left foot,” etc. The only way we could teach her to do something like skipping or galloping was to break it down into slow motion with verbal cues.
When Emily began sensory integrative therapy, she seemed to respond best when the occupational therapist introduced linear movement, such as forward-back or side-to-side in small excursions and on low lying equipment. She was more accepting of these movement activities if the therapist held her firmly and physically guided her through the movement. At home, her parents found that they needed to be very gradual in their approach to Emily, starting with activities that were close to the ground. For instance, they found that Emily could tolerate movement while sitting on their laps and rocking together while they pretended that they were traveling in a spaceship or boat to different places. It was important not to impose vestibular stimulation on her because it could be more disorganizing than integrating. Slow, rhythmical movements were used. Emily liked it when her parents moved with her slowly in creative movement to music with strong drum beats and nature sounds. Emily also responded well to these movement activities if she had visual or auditory cues to orient where to look as she moved.
At first the goal was very simple—to just touch moving equipment or to put a favorite toy on the swing. When her parents took her to the playground, they would bring a favorite stuffed animal and watch it ride on the see-saw or swing first, then Emily could be coaxed to ride with it. In this way, she gradually learned to tolerate the visual component of watching the movement before she was expected to move in space. After several months of occupational therapy and a home program, she was spontaneously climbing on playground equipment and did not display the fear that she originally experienced. Balance and motor planning skills began to improve.
Vestibular-based dyspraxias: The most common types of motor planning disorders observed in children with vestibular-based problems are related to postural, sequencing, bilateral motor coordination, motor planning, constructional, and praxis to verbal commands. Treatment should focus on the ability to plan whole body movements in space and to combine the body with objects. Through the use of postural patterns of flexion and extension against gravity, trunk rotation, and diagonal rotary patterns, the child can learn to map simple body movements in space. These postural patterns should always be combined with functional activities so that the movement pattern has a purpose for the child. The body flexors are the mobilizers while the extensors are the stabilizers, therefore, flexion is often needed in children who have troubles learning how to initiate movement patterns. These whole body patterns should be used first before small skilled movements are attempted (i.e., cutting a play doh snake with scissors). Activities should use vestibular-proprioceptive sensory stimulation in combination with a strong visual component to help the child to see what he is doing in space and to visualize the effect his actions have on objects. For example, by having the child sit in a hammock and swing to kick over a tower of cardboard blocks will give him vestibular, proprioceptive, and visual feedback to consolidate the motor plan of kicking over the tower. The major emphasis is therefore placed on relating the body in space in relation to objects. Activities involving motor accuracy (i.e., throwing velcro balls at a target), bilateral motor coordination, and sequencing of fine and gross motor movements (i.e., skipping, cutting out a triangle) should follow treatment directed toward basic postural patterns.
10. Case example of treatment approach with child with pervasive developmental disorder
In this example, the treatment process of a young child with pervasive developmental disorder is presented to illustrate how sensory integrative therapy and child centered activity are blended in treatment with emphasis on developing the child’s social relatedness through the parent-child relationship.
Sandra was a 2-year-old child who was diagnosed as having a developmental delay with autistic-like symptoms. She had had a medical work-up that ruled out genetic and neurological disorders and had not yet had early intervention services. Her parents were hoping to gain a better understanding of Sandra’s problems and how they might begin to help her.
Sandra’s parents first became concerned about Sandra when she turned 1 year of age. They noticed that she was not making eye contact or pointing to body parts or objects like their older, 4-year-old daughter had done at that age. By 15 months of age, they alerted their pediatrician that Sandra was not talking. By 18 months, they expressed concern again about her talking and were told that if she did not begin talking by 2 years, her hearing should be checked. The parents did not want to wait any longer, and at 22 months, they began investigating the nature of Sandra’s problem.
10.1. Presenting concerns
Mr. and Mrs. T. came to the intake interview to discuss their concerns about Sandra. She had no words but could make sounds, sometimes in a social context. For example, she could make an “aaaaah dadada” sound in greeting. Her sounds tended to be high pitched with short bursts of screams. She vocalized the most when she was in front of a mirror. If she wanted to communicate a need, Sandra would cry. Sometimes she would move her mouth with great effort as if she were trying to say something. Sandra could imitate mouth and tongue movements, such as sticking her tongue out and she could make simple sounds. She was not able to follow any commands although she understood the meaning of “no.” If touched by her parents after a command was given, Sandra had an easier time following through although this was inconsistent.
Sandra’s favorite play activities were playing pop-up pals, rolling balls, twirling or swinging string, dragging fake pearls on the tile floor, listening to music, looking in mirrors, and watching Sesame Street videos. She loved music and would jump up and down or wave her hand while she listened. She appeared interested in making sounds with objects. For example, when she hit the string of pearls on the floor, she created different types of sounds. She carried the pearls about with her, almost as a source of comfort like “worry beads.” Sandra would spin dishes, dump objects, or throw toys. She was fixated on strings and would go to great lengths to find them, pulling threads out of a rug to put in her mouth. Mr. and Mrs. T. reported that she had few imitation skills and no symbolic play. There was little turn taking ability although her father stated that he could get her involved in a reciprocal game of rolling the ball. Wandering occurred almost constantly. Sandra would mouth toys and would try to eat or chew on books. Sandra was most connected with another person during singing activities. She also enjoyed hide and seek and peek-a-boo games. Sometimes she would pinch others, especially if she was angry or jealous when her older sister was sitting with her mother.
Sandra was a picky eater with definite food preferences. She had just begun to use a spoon or fork. When she did not like the food or was finished, she would throw the plate or cup on the floor or against the wall. Usually, Sandra would handle or feel the food with her fingers before eating it. During mealtimes, Sandra was whiny and had a hard time sitting still.
Sandra experienced a range of sensory hypersensitivities. She would cover her ears when she heard unusual sounds, such as an animal noise or the videotape rewinding. Sensitivity to light was noticed when she would squint vigorously when outside in sunlight. Sometimes Sandra enjoyed being held but she didn’t hold onto her parents when they hugged her. Instead, she would bury her hands under her body and act as if she was just putting up with being hugged. She didn’t hold onto a person’s hand when being led someplace. She loved swings, riding in a stroller, and jumping in the crib. Motor planning problems were noted in certain situations. When coming downstairs, she would scoot on her bottom rather than holding onto the rail and walking. Sandra enjoyed visual stimulation, such as looking in mirrors, watching reflections and shadows, and creating visual effects with a swinging string. She also loved music and making sounds with objects.
10.2. History
The pregnancy was planned and uneventful with no complications. Sandra was born full-term after 6 hours of labor via vaginal delivery. She had been healthy except for one ear infection. Sandra was big for her age, falling at the 95th percentile for height and the 90th percentile for weight.
Motor development was reported to be on course. Sandra walked at 13 months although her parents stated that she was more content to sit than move about. She smiled at 4 months and engaged in games like peek-a-boo as a young baby. Communication, play, and social–emotional skills were delayed for Sandra. Her parents suspected that she might be bright. For example, she understood where things were in the house and appeared to remember events.
Both parents were unsure about the future for Sandra. They had been told that she would probably need “special education services forever” from various doctors. They had just begun the process of identifying her problems and had been focusing on her medical diagnosis. They felt that Sandra had potential and that she was smart, but did not know how much she would progress.
10.3. Clinical findings
A variety of clinical observations and tests were used to help delineate the nature of Sandra’s problems. When observed in play, Sandra engaged in aimless wandering, a behavior that also occurred at home. She seemed most interested when given toys that involved the sense of touch (e.g., koosh balls, paint brush). She was not able to engage in symbolic play, and vocalizations only occurred during play with textured toys. Although Sandra was reported to enjoy movement, she did not want to move on the various pieces of moving equipment that were presented to her in play (e.g., inflatable bolster). She was unable to engage in reciprocal interactions, nor did she respond to her mother’s attempts to interest her in particular toys or herself. The only time Sandra responded to her mother was when she was told “no” to mouthing toys. Her affect was quite flat and eye contact was fleeting.
During testing for cognitive and language skills, Sandra mouthed all of the objects presented to her. She only stopped mouthing when her mother cautioned her, “Not in your mouth.” When she manipulated objects in her hands, she often rubbed them on her face, and at times, waved her arms back and forth across her body, or flapped her hands while holding the toys. Sometimes Sandra seemed angry or frustrated, throwing things on the floor or refusing to cooperate. She especially liked the red ring on the string and anything that was shiny like the mirror, bell, and spoon. Most of her sounds were vowels, squeals, or grunts. Although testing at this age for children on the spectrum can be unreliable, her overall functioning was about at the 8 month level with scatter to 13 months. Her best skills were fine motor and simple problem solving. Language and social skills were the most difficult for her.
10.4. The treatment plan
The goals for the treatment were as follows:
1. Develop social engagement and basic communication skills:
a. Facilitate Sandra’s toleration of being near other people without the need to escape or wander away. Explore what sensory modalities (i.e., tactile-proprioceptive, vestibular, auditory, or visual) would help Sandra to sustain social engagement with others.
b. Help Sandra to give signals of what she wants by creating play experiences that made it clear to her that her gestures or sounds created an effect on the environment and a reaction from other people.
c. Develop the capacity to tolerate face-to-face interactions, exploring what types of activities support eye contact without avoidance or overstimulation (e.g., focusing on tolerating sitting side by side to parent).
d. Once social engagement and gestures emerged, emphasize reciprocal interactions through turn taking.
e. Establish social routines in everyday life that Sandra can predict and facilitate communication around those events.
2. Develop the capacity for more varied and adaptive responses during object and social play with more elaborated attention to the task or person.
a. When Sandra was engaged in a stereotypic or repetitive activity, challenge her by introducing a conflict, element of surprise, uncertainty, or complexity to the task or interaction that forces her to engage in a different response.
b. Find the balance in the level of stimulation in the task, the way the environment is structured, and how the parent interacts with Sandra so that she can tolerate the stimulation and engage in an adaptive response without becoming disorganized, avoidant, or overstimulated.
c. Employ the use of activities or materials that give an obvious beginning and an end so that it is clear to Sandra when she has successfully completed a task, or engage in simple interactions that are predictable (i.e., game of hiding the ball under mom’s shirt). Once Sandra can remain attentive to a simple activity, expand on the steps that need to be taken before the task or game is completed.
10.5. The treatment program
Both parents came to the first treatment session, after which the father attended the remaining sessions until the very end of the treatment program. Mrs. T. experienced a great deal of sorrow and distress about her daughter’s impairment and her adaptation was to remove herself from the intervention process until Sandra began to show progress. At the time that the therapy program was initiated, Sandra was placed in a local school system early intervention program.
Our focus at the beginning of treatment was on the integration of sensory integration therapy and child-centered play. Sandra became easily overstimulated by being in close proximity to her parents, and constantly ran away from her parents as we attempted the child-centered activity. Another important part of the early work was to help her parents to become comfortable with this approach, as both preferred a highly structured, teaching kind of approach with Sandra.
10.5.1. The first session
On the first session, Sandra reacted to the child-centered play by running and fleeing from her parents. She was accustomed to playing alone or wandering about the house aimlessly. I suggested to Mr. and Mrs. T. to try to make it a game of chase, saying “Got you,” then catch her with their arms or by using a hula hoop. Most of the session was spent with her parents running around the room after Sandra. We found that if they sat in one spot and didn’t move, Sandra shut them out completely. Later in the session, she became interested in playing with some plastic balls that were in a wading pool. I suggested to Mrs. T. to hold out a ball in her palm for Sandra to reach. When Sandra tried to grab the ball, Mrs. T. gave the ball a little tug or resistance. When this happened, Sandra started to look at her mother’s face. At other times the slight resistance frustrated her, and on one occasion, Sandra tried to bite her mother’s hand.
At the end of this first session, I debriefed with Mr. and Mrs. T. about what we learned about Sandra. They were puzzled by how following her lead would help. I suggested that they try to get on Sandra’s level and figure out what she was getting out of the activity. This was very upsetting for Mrs. T. She felt great sadness for Sandra and said while choking back tears, “I entered Sandra’s world today and I don’t like what I see.” In the upcoming weeks, Mrs. T. became very depressed about Sandra’s diagnosis and stepped out of the treatment for the next few months until Sandra began to make progress. In the meantime, Mr. T. came religiously to each week of treatment, showing an intense desire to help his daughter. I urged him to give his wife space as she coped with the emotional meaning of what was going on with their daughter. I also pointed out that it’s not uncommon for a couple to have different responses to learning that their child had autism.
10.5.2. Session #2
On the second week, Mr. T. asked why Sandra ran away from them when they came near her. He interpreted it as rejection. I talked about how Sandra had difficulty tolerating the sensory stimulation of having another person in close proximity to her and was probably overwhelmed with the interactions of another person. Sandra engaged in play with bean bags and seemed to organize herself when sitting inside of an inner tube with her father. She was able to tolerate her father’s proximity for short periods of time. Sandra tended to look at father’s face through the mirror rather than face-to-face, so I encouraged Dad to engage using the mirror as the go-between. There was more eye contact this week and less avoidance or running away. This week I made several suggestions for child-centered therapy to try at home and wrote them down so that Mom could be included in the process if she so desired. Here is what I gave them:
1. Provide things that Sandra can roll on (like the bed or a rug) or objects that she can touch (legos, koosh balls, bristle blocks). If she likes something like the bristle blocks, hold the bag so that she has to come to you to get them.
2. Imitate her actions, if she stomps her feet, do the same with her.
3. Since Sandra seems to like your rubbing her back, try laying down facing her while you do this. Start rubbing her back, then see if she indicates that she wants more.
4. Label her gestures “push,” “jump,” “give” when she does them.
5. Sandra likes when you create a space for her that she can sit inside of—like facing you with your legs out straight or in an inner tube or wading pool filled with pillows.
Mr. T. reported noticing that Sandra played differently with each parent. Dad felt that the play went better with him than with his wife. Although they did not seem to be competitive with one another about the play, I reminded him that children normally play differently with each parent because of their unique meaning for the child.
10.5.3. Session #3
Mr. T. was delighted to report that Sandra, after just 3 weeks of therapy, was not avoiding him when he engaged in play with her anymore. She tolerated being face-to-face most of the time. He found that if they played on the bed with pillows, rolling about and rough housing with each other, Sandra would become very animated. She continued to enjoy looking at herself and her parents in mirrors. She played among other children one day, eating a snack with them which she had never done before. For the first time, Mr. T. noticed that Sandra was starting to notice her older sister. This week she smiled at mom and dad several times—a first! In the treatment, Sandra looked at her father on several occasions. For example, her father walked away from Sandra to take off his jacket, and Sandra looked at him almost insistently, like “Hey, get back over here!” She had stopped running away and avoiding interactions. Sandra was still mouthing toys, but we saw more purposeful manipulation, feeling textured koosh balls in her hands. Her best play was when she was playing with the plastic balls in the wading pool and sliding down a small slide into the balls. Dad and Sandra played a little tug of war with the plastic balls on several occasions, a game they both enjoyed. To help Sandra tolerate looking directly at father’s face, I suggested holding an object up in front of Dad’s face (e.g., two plastic balls in front of his eyes). This week Sandra gestured and vocalized when she was frustrated when something was taken away from her.
Dad was encouraged by some of the changes he was seeing, yet he expressed the worry that Sandra was not showing improvement in language. I assured him that Sandra was making steps in that direction by looking more at him, tolerating the proximity of the interaction, and protesting when she was angry.
10.5.4. Session #4
Dad spent most of the time talking about the alarm his wife and him felt at seeing Sandra in the special school setting with other “autistic” children. They felt that Sandra was very different from the other children and seemed more impaired than them. She was very tired from her day at school and when she came to therapy that afternoon, her attention span was very short and she spent most of her time mouthing toys. After about 10 minutes of play, she wanted to be cuddled by her father. When we talked about how the play had been going at home, Dad stated that Sandra was looking much more at them and drawing them into her play, particularly when they did rough housing on the bed, something that she anticipated and enjoyed. The tactile toys continued to be the ones that attracted Sandra and seemed to organize her the most.
Dad discussed how he was feeling that he needed more time for himself, that he had been very busy with work life and driving Sandra to therapy. Mom continued to feel depressed about Sandra’s prognosis and found that when she did the child-centered play at home, she became upset. I asked if the parents had time to talk about their feelings about Sandra, that many parents felt a deep sense of loss and grief when they learned that their child has problems and that many are afraid of what the future might hold for them and their child. Mr. T. said that he and his wife coped by busying themselves with everyday tasks rather than talking about it. He felt that when they talked, they both got depressed and one of them needed to be able to mobilize and get Sandra to the therapy and school. I supported him on what helped them most at this time.
10.5.5. Session #5
The next week, we found Sandra to be very clingy of her father now that she was going to school 5 days per week for half-days. The school program was using a behavioral approach that stressed complying to requests and following commands. Sandra was very tired after school and wanted to be cuddled the whole session by her father. She was so exhausted that we were unable to attempt the play. At home, Sandra was looking at her parents more. The teacher also noticed better eye contact. I discussed how the next step for Sandra was for her to tolerate and want to play with her parents. This was already beginning to happen in her anticipating a few new favorite toys and the rough housing game on the bed. I suggested that Sandra would need to rest after school, but to keep the CCA going. If she became avoidant and ran away, I encouraged them to pursue her during the play time. I suggested sitting a distance away from her and see if she looked at them, then go to her to make it clear that she made them come to her by looking at them.
This week, Mr. T. talked more about how he and his wife were feeling. They both felt anxious about Sandra’s future and wondered what was really wrong with her. They were feeling very stressed with work, meeting with teachers, and keeping all the appointments. We discussed getting some respite. Dad’s mother lived locally and could help with some of the tasks that needed to get done. I reinforced how the parents’ hard work doing child-centered therapy had already resulted in many changes for Sandra. I encouraged him to not let this be the thing that they let go of in terms of home activities. I stressed that the child-centered play was like giving a child a daily dose of vitamins. I asked him to think of what task he could defer or delegate to alleviate the burden. He left the session hoping to sort this out for himself.
10.5.6. Session #6
This week Sandra showed a great deal of eye contact, initiating games of peek-a-boo. There was a little wandering through the play, but her object play was much more purposeful. She seemed to like heavy toys, textured toys, and games involving movement. These types of toys helped Sandra to engage in interactions with her father. I observed Sandra to be much more responsive to her father’s signals, and smiling and laughing more. Her ability to sustain the play was wonderful with focused attention for both her father and the toys. The game of chase that we had started in the early weeks was now a real game of interaction where Sandra would look at her father in anticipation of being caught. There was no longer an avoidant quality to the running from her father. Dad played a game with Sandra where they each held an end of the slinky and jostled and stretched it about, remaining connected to one another through the slinky. I suggested trying stretchy ropes or old panty hose, slinkies, or hoops at home that could be used in a similar way. Sandra also seemed to enjoy the game of giving and taking the balls from one another. Dad would hide the balls in his hands, under his shirt and exclaim, “Where did it go?”.
10.5.7. Session #7
In the upcoming weeks, the emphasis was on helping Sandra focus her attention, engage in reciprocal interactions, refine her gestural and vocal signals in interactions, and to make use of sensory stimulation without becoming overwhelmed. Sandra could only sustain her attention for about 30 seconds to 2 minutes for activities that she found interesting. Here are some of the things that helped her stay focused:
1. Deep pressure applied to Sandra’s back, hips, or top of her head with the parent’s hand. This seemed to settle her during activities so she was less apt to run away and to help her to be more able to stay with the task.
2. Giving her pillow hugs by wrapping the pillow around her back and giving her a squeeze, or letting her lie on a thin foam mattress or sleeping bag and fold it over her to make a sandwich with her inside seemed to organize her. The goal was to have her look at her parents in an interaction or to help her calm and focus her attention better for the next activity.
3. Giving Sandra a ride while prone or sitting on the large therapy ball using a rhythmic movement elicited lots of smiles and eye contact. I encouraged the parents to stop the bouncing or rocking and wait for her to indicate “more” by a look, gesture, or vocalization.
4. Singing short songs while mom and Sandra moved together was fun. I encouraged Mr. and Mrs. T. to use their trampoline at home to jump and sing with her while they held hands together. I also suggested that they pick songs and repeat them over again so that Sandra could link a song with a game.
5. Sandra liked a carpet ride on a towel while she laid prone. Dad learned to stop the ride and wait for her to indicate “more.”
6. To help Sandra with her attention, I suggested to confine her space and limit distractions by having her sit in an inner tube, under a table with a cloth over the top, or in a refrigerator box filled with pillows. When inside these spaces, they tried looking at a book with a flashlight, playing pop-up pals, singing, listening to a tape player, or playing with the vibrating toothbrush on her hands, face, or feet. She also seemed to like searching for her favorite doll in the box. In all of these games, I encouraged Sandra to initiate the activity, then have her parents respond to her after she took a turn.
7. I expanded on the mirror play to include an activity like smearing crazy foam with their hands or a paintbrush, or picking stickers off the mirror.
8. I also suggested keeping fewer toys out at a time at home and to work on attending activities for short chunks of time.
Mr. T. expressed his concerns that Sandra’s attention span was very short for activities. Techniques that we discussed, such as enclosing her space, such as sitting in a refrigerator box were viewed as drastic and “abnormal.” He feared that Sandra would always need these things. I tried to support the notion that Sandra’s progress was attributable to what they as parents were doing, not some magical techniques that a therapist might try. On a few times during the session, Dad was visibly upset as he watched Sandra, tears welling in his eyes. He expressed fears that even when professionals tried things, they were struggling to figure out how to reach Sandra. Could anyone reach her? Mr. T. felt that Sandra was showing a period of regression where she was twirling strings repeatedly, pulling strings out of the carpet, and finding them anyplace she could. The parents could not take the strings away fast enough to prevent the behavior.
10.5.8. Session #8
Sandra was most attentive when there was intensity in sensory stimulation—loud sounds, vigorous movement, or deep touch-pressure. By nature, Mr. T. was a quiet person and had trouble expressing exuberant sounds like “Weeee” as Sandra would ride down the sliding board. I encouraged him to try even if it was hard for him because it got, such as good response from Sandra. I saw a lot of excitement and pleasure in the sensory activities that we tried like kicking a ball with her feet while sitting on a swing. A few times Sandra initiated interactions or showed her wants by pursuing a toy or bag of crackers. Most of her communication was still bound by actions rather than using gestures or sounds. Once in a while she would say a word, that is, “Up” and raise her arms. At home, she had just started greeting her parents at the door when they came home after an errand or from work. In all of the activities, I stressed the importance of two-way communication, refining gestures and signals, and taking turns.
During the debriefing after the play activities, Dad talked about how Mom was involving herself in cleaning, shopping, and other household tasks. Dad continued to feel that he had little time for himself to refuel. I stressed the importance of time and pleasureable activities for himself. He wished that he had time to go out to play basketball with a group that he used to play with on Monday nights. I encouraged him to do this and stressed the importance of each parent taking time for themselves.
10.5.9. Session #9
Dad reported that Sandra was engaging in perseverative behavior again with the string twirling. He was worried that Sandra was regressing. I suggested that Dad try to enter into the string play by grabbing the other end and tugging, covering the string up with his hand, or some other way to get some variety in the play. Apparently, Sandra would look desperately for more strings and would pull them out of the carpet if they were taken away from her. Despite this, her parents had started a game of playing ring-around-the-rosey that Sandra loved. Sandra spent the first part of the session running about the room, after which she was much more interactive and communicative. I dimmed the lights to help decrease her overstimulated state while running. After the motor discharge, she was able to engage in many circles of communication, looking for an object hidden in Dad’s hand repeatedly or playing ring-around-the-rosey and asking for it again and again, clapping with delight, then grabbing our hands for more. I felt that Sandra was showing great strides in her social interactions, but that she also needed help with modulating her overarousal. The behaviors that father reported at home were worrisome because Sandra was regressing into a maladaptive pattern to regroup rather than seeking a more purposeful and productive outlet to self-calm.
10.5.10. Session #10
This week Sandra’s gestures were a bit better. It was possible to wait for Sandra and ask, “What do you want?” and she would either tug her father and point to what it was or would vocalize a sound for something. I suggested giving Sandra choices at mealtimes, such as, “Do you want the cookie or the juice?”, holding each choice up for her to pick from. I brainstormed games that had obvious beginnings and ends to them like the ring-around-the-rosey, or kicking a ball into a can. I also discussed social interaction games that Sandra would enjoy, such as putting funny sunglasses, hats, and stickers on her face and her parent’s faces.
10.5.11. Session #11
Sandra showed a strong need this week for movement, firm deep-pressure, and vibration to help organize her attention. An electrical vibrating massager was very intriguing to Sandra, holding the massager up to her face, then to her father’s. Her attention was getting longer, staying with tasks for up to 5 minutes each. She particularly enjoyed games with the magnetic balls and wand.
This week, Mr. T. talked more about his fears about what the future held for Sandra. Despite his worries, he persisted in trying all of the activities that had been suggested over the course of the intervention. He stated that Mom was now getting involved again in the home program and was noticing some changes in Sandra.
10.5.12. Session #12
On the last week of the intervention program, both parents came and talked about how Sandra was responding to them when they gave her choices about toys and food. For example, they were holding up two different toys, two different videos, or two food choices and Sandra could point or vocalize. They were also able to get her to communicate “more” with a game using the bubbles. The mother would recap the lid on the bottle and wait for her to indicate her desire for more bubbles. Sandra now enjoyed interactive games that had bouncing or clapping while the family sang or listened to music. She continued to respond well to tactile activities, such as riding on the blanket and rolling up in the mattress like a hot dog. Both parents played with Sandra this session and were able to get her to complete multiple back and forth interchanges (i.e., “circles of communication”) by hiding toys and getting her to pursue them, chasing games, play with the bubbles, and singing and movement games. Sandra appeared particularly happy having both parents there, smiling and laughing as she played with them.
Mom appeared much more upbeat this session and talked about what a hard time she had had in coping with Sandra’s diagnosis. Both parents were very worried about her future but felt that she had made substantial gains. They believed that Sandra could be reached and that she was related and interested in people. They felt less like Sandra was in her own little world. I acknowledged the hard work that they had put into the therapy process that resulted in these changes. I talked about what Sandra needed to continue her progress and what had worked most in the treatment. They felt strongly that the sensory activities helped to support her attention, communication, and interactions. I also talked about getting this type of therapy in the school program and how they would need to advocate for this since their program was very behavioral in nature.
10.6. Conclusion of treatment
Sandra was a child who showed many traits of pervasive developmental disorder. Those things that challenged her most were in the areas of social interaction, engagement, attention, sensory processing, and basic communication. In the therapy program, the child-centered therapy helped her to become engaged, tolerating the proximity of her parents to her while playing. She was beginning to initiate purposeful actions and was less repetitive and stereotypic in her play behaviors, and she began to engage in more reciprocal interactions. In the second half of the therapy, I introduced more structure into the therapy program while elaborating on the core principles used in child-centered therapy. The most success was in finding sensory activities that supported her attention, interactions, and communication. Gains were made in gestural and vocal communication, turn taking, attention, and sensory modulation. Sandra was less apt to become overwhelmed by the level of stimulation and, by the end of the treatment, could find adaptive activities to engage in rather than stereotypic, repetitive, or regressed activities.
This case depicts the importance of respecting how the parents feel as they cope with their child’s diagnosis and what it means for them and their child. It was important for me to respect the grieving that each parent experienced, allowing them time to adapt while providing opportunities for them to express their concerns and supporting them in ways that helped. Integrating this piece into the treatment was just as important as providing practical guidance, sensory integration techniques, and child-centered activity in helping Sandra become more related to the people and object world.
11. Case example of a child with severe sensory defensiveness: therapy spanning from infancy to adulthood
My work with this case began when Ali was 9 months old and spanned the course of 21 years. Working with Ali has given me a longitudinal perspective to observe what works and what doesn’t work in the treatment process, but also the opportunity to understand how severe sensory defensiveness evolves as the child grows older and its impact on emotional development. Ali’s symptoms early on were typical of the regulatory disorder described as the “fearful and cautious” type. Early on Ali’s symptoms included severe sensory defensiveness, hyper vigilance, fearfulness of people and sensory phenomenon, and clingy, dependent behaviors. Although she was an easy baby, high irritability and crying emerged in the second year of life. These symptoms evolved over time into a child with oppositional/defiant disorder and persistent sensory defensiveness. Although Ali improved significantly over the years in her sensory integrative disorder, she was diagnosed in the preschool years as also having nonverbal learning disability. What is very interesting in this longitudinal case is to take a look at the transformation of symptoms that occurred in Ali from a fearful/cautious child to one who fluctuated between a state of emotional and physical shut-down to oppositional defiant behavior. This case description will also explore the impact of Ali’s regulatory disorder on the parent-child relationship and the importance of addressing both constitutional and parent-child relationship dynamics in the treatment process.
11.1. Ali at 9 months
I first met Ali at 9 months of age when her mother brought her in as a control subject for my fussy baby research study. I remember Mrs. B. telling me how proud she was to bring her baby as an example of “normal.” The assessment process included assessment of mother–infant interactions, temperament, parental stress, and self-regulation, as well as testing for sensory processing and attentional problems. In the play observation with Ali and her mother, it was striking how immobile and inactive Ali looked. Here was a 9-month-old who was content to lie prone on the mat, not reaching for toys or moving about. She was watching the world go by. Her mother seemed attuned to Ali’s vigilant state and commented on what Ali was looking at. When Ali reached for a toy, Mrs. B. would ask Ali, “What’s that?” or she would prompt Ali to do things with the toys like “Shake the rattle!” Testing showed that Ali was slightly behind in all of her skills. She was also highly defensive to touch, recoiling when I touched her on her arms, hands, face, or legs during the Test of Sensory Functions in Infants. When I moved her about in a simple rough house routine, a part of the TSFI, her body stiffened abruptly, her arms retracting, and she cried. She couldn’t tolerate me moving her in a simple up and down movement of her body in space. She seemed reluctant to touch appealing toys and when she did touch them, the toy remained inert in her hands. It seemed that a combination of tactile hypersensitivities and motor planning problems made it difficult for her to touch and plan simple actions with objects.
Although Ali seemed to have an easy temperament, she was too easy, passive in receiving the world and needing her parents to bring the world to her. There was clearly something more behind her “easy” temperament—most likely a chronic state of sensory overload and emotional overload. She was slightly behind in her development, and because she had problems tolerating touch and movement, and was not exploring the world, I suggested that it might be useful to provide Ali with some input to help her with these areas. Mrs. B. did not want to hear that her daughter might have problems. I expressed my interest in seeing Ali at our next follow-up visit at 2 years, and urged Mrs. B. to feel free to call me anytime if she had any concerns. I was aware that my feedback to Mrs. B. might have alarmed her, shattering her view that she had a “normal” baby. I wasn’t sure that she would come back to see me, but before it was time for the 2 year visit, Mrs. B. called me, feeling urgent that she get help for Ali.
11.2. Ali at 2 years
When Mr. and Mrs. B. brought Ali for the two year visit, they were desperate. They couldn’t take Ali anywhere without her becoming extremely distressed. She would cry and cling in terror to her mother when they went to family gatherings, play groups, and visits to the store or playground. Ali appeared panic stricken in groups, trembling all over, clutching a tattered blanket and saying repeatedly, “Go home, go home.” Mr. and Mrs. B. had given up on going many places and were feeling that their world was becoming increasingly more restricted and isolated. Grandparents and relatives often asked “What is the matter with that child?” and offered unwelcome advice about what they should do instead. Not only were Mr. and Mrs. B. feeling shut off from the world as parents, but they felt at a complete loss for what would soothe Ali. Once upset, she was inconsolable, clutching frantically at them.
Mr. and Mrs. B. reported that Ali was unable to tolerate other children being near her, even at a distance. She seemed in terror of their activity level and noise. Ali could not stand to be touched, making daily tasks, such as dressing and bathing a nightmare. Despite this, she wanted to be held constantly for comfort when distressed. It seemed that the only kind of touch that she could tolerate was static– being held but not stroked. She would touch objects, but only on her own terms. She avoided movement activities like swings that most children her age enjoy. She was bothered by noises, noticing sounds that most persons don’t normally notice. She would become extremely distressed by vacuum cleaners, sirens, bells, or toilets flushing. Ali was showing many of the characteristics of a child with sensory defensiveness, but it was accompanied with severe anxiety as was evidenced by her strong emotional reaction to group situations and leaving the house.
When I saw Ali for testing at 2 years, she could not sustain interest in toys, playing only briefly before losing interest altogether. She was very cautious in exploring the toys, generating play only when cued by her mother what to do. While holding a doll, her mother prompted her to point to the doll’s body parts. Ali was not able to initiate or organize any symbolic actions with the dolls, things like feeding the doll which most 2 year olds can do. Although her cognitive and language skills were within age expectations, Ali’s play was restricted to labeling objects or defining the objects’ properties (i.e., what color it was) and she wouldn’t play unless her parents organized it for her. Ali was experiencing a significant motor planning deficit, attentional problems, difficulties organizing reciprocal interactions, and problems using language for communication.
Here was a child who, at age 2 years, was still clinging to her parents, fearful of exploring the world, and unable to organize even the simplest of play. The task of engagement with others was seriously compromised by her fear of social approach by others, her sensory defensiveness to touch, sound, and movement, and her limited capacity to sustain interest in persons and objects. Although she clung to her parents, her attachment to them was highly anxious. She had not learned to negotiate the basic task of engagement and intimacy with them. She had created a state of being merged with her mother that was unpleasant and intolerable for her mother. Mr. and Mrs. B. found themselves pushing Ali away when she clung to them. It appeared that Ali was not yet ready for the task of separation and individuation.
During the assessment I asked Mr. and Mrs. B. to step out to the observation booth so that I could see how well Ali could separate from them and soothe herself. Initially Ali was very upset and cried, but she comforted herself by standing against me while holding her blanket. After a few minutes, she became interested in playing with toys, and began interacting with me around them. It appeared that Ali had some capacities to separate and when she could do this, she was better able to construct purposeful and organized play and reciprocal interactions with me. It seemed that Ali and her parents were stuck in a conflict—Ali wanted her parents to soothe her, but they resisted this task—pushing her away and until Ali felt that her needs for closeness were met by them, she would persist in this position—to cling, cry, and insist on being “one” with her mother. The severe sensory defensiveness was one of the reasons that Ali experienced caused her to be stuck in this dynamic.
11.3. The treatment at 2 years
My initial treatment plan was to focus on working through the parent–child relationship to address Ali’s constitutional and regulatory difficulties. Although she would have benefitted from occupational therapy interventions right away, I decided to focus on helping Ali to self-sooth, developing an attachment between mother and child, and learning how to explore the world without becoming overwhelmed before making that referral. Addressing the emotional aspects of the parent–child difficulties that existed between parent and child were central for her treatment. During therapy sessions, child-centered therapy was practiced for about 20 minutes between Ali and her mother or father, followed by a discussion about the process. My goals in working with Ali in this way were to facilitate self-initiation and problem solving, motivation to explore the environment, better sustained attention, better signal giving, sensorimotor exploration, a more secure and joyful attachment to her parents, and a broader repertoire of parent–child interactions.
When we began the child-centered therapy, Mrs. B. expressed feeling conflicted about the way in which we would be working. She had seen a psychologist before coming to see me who counseled her not to pick Ali up when she cried. In our first treatment session, Ali cried vigorously, wanting to be picked up, clinging to her mother and asking repeatedly to “go home.” I suggested to Mrs. B. that she allow Ali to self-initiate and indicate what she needed. She was asking mother to nurture her, to hold her, and comfort her. I explained to Mrs. B. that Ali needed to feel comforted by her mother in a basic way, like a young infant, and she needed to experience this before she would become self-reliant in soothing herself. Mrs. B. was upset by Ali’s distress and did not want to hold her. When she held her, there was a pained expression on mother’s face. She felt that all she did was hold her and did not think my idea would work. I suggested that when we practiced the child-centered therapy, Mrs. B. would learn how to read Ali’s cues, to respond in ways that Ali needed, while at other times she could set limits (e.g., “no holding right now, I’m cooking dinner”). When I asked her what bothered her so much about holding Ali, she expressed that Ali was feeling abandoned by her. This was probably a very real experience for Ali because Mrs. B. expressed that she did want to escape from her child. Mrs. B. talked later in the session about wishing Ali was different—singing and playing like the children she heard through the wall in the next room. She also told me that she was uncomfortable being observed by me while she interacted with Ali. I was struck by how she wanted the ideal child who others would admire, yet it was difficult for her to share how painful their relationship felt to her.
In the following week, Mrs. B. reported that she had had a good week with Ali. They went to several outdoor events and new places without Ali becoming distressed. Despite this positive change, Mrs. B. expressed how helpless she felt when Ali became distressed and how vulnerable Ali must feel. That week in therapy, Ali wanted to be held the entire time, but she didn’t cry. She listened to the children in the next room and even laughed as they sang songs. She experimented making loud sounds by kicking a chair. We ended the session playing a game of hide and seek with a toy to begin working on separation using a neutral object.
Over the following weeks in treatment, Ali remained clingy to her mother in the waiting room. Her crying and distress improved, but she continued to use her mother as a calming object, stroking her mother’s hair. Mrs. B. reported that Ali was beginning to use transitional objects like a toy or blanket, however, sometimes her selection of an object was odd like carrying an onion around with her. She used these objects to stay calm in new situations. We had intermittent success in the next few weeks—a play date at another child’s house that went well, then Ali screaming on another play date. Her parents were angry at her that she was this way, seeming to expect a quick fix. Mrs. B. was distressed that Ali was so dependent on her. Mrs. B’s own parents did everything for her as a child and she wanted Ali to be more independent. To respond to Mrs. B’s wish for Ali to become independent, I suggested that she give Ali jobs to do like turning on the light or picking out a toy to play with as they entered a room which would also serve to organize her.
Within a month of the start of treatment, Ali began to readily approach me. After picking out toys that she wanted to play with, Ali would rock in a chair, climb the ramp and look in the mirror and engage in other movement games like chasing a large ball, but she did not interact with any toys. Gradually she began to play with various toys at my office during the child-centered play, selecting things she could throw. I put out koosh balls, heavy bean bags, and other safe medium to throw that would provide her with tactile-proprioceptive input. Sometimes Ali would become overly exuberant and wild, throwing koosh balls around in her play. Because of the level of dyspraxia that she experienced, I would sometimes model things like a simple symbolic play scenario. If I showed her how to do it, for example, feeding dolls with play doh, she could imitate me and seemed to enjoy enacting these schemes. However, whenever I introduced a doll into play, Ali would react as if it were real. For several weeks we had to have the doll just present in the room to get her accustomed to it.
The child-centered therapy was completely different at home. When her parents practiced it. Ali would want to hold an object that was unsafe or she would stop playing after only a few minutes. I was aware that both Ali and Mrs. B. needed me to contain their relationship. It seemed that Ali tested her mother by expressing unsafe or impulsive urges. Her parents also expressed a lack of pleasure in being with Ali and could only experience more positive interactions in my presence.
In the upcoming months, Ali gradually stopped asking to “go home” when out on excursions. She began testing limits more by running off or putting things she shouldn’t into her mouth. She was going to a play group with 2 children and doing well, but when she fell apart, Mrs. B. interpreted it as a major setback. Mrs. B. felt that other mothers viewed her as a bad mother and that something was seriously wrong with Ali for her to behave this way. Mrs. B. expressed strong feelings of isolation, depression, and hopelessness. She worried that Ali would always be this way. It pained her that Ali avoided people. She thought about quitting her job and moving away. Her only contact with others was seeing me or the play group once per week.
In addition, there was enormous strain on her marriage. Mrs. B. would call dad whenever she had had it, wanting him to come home immediately. It was clear that containing her own distress was difficult for mom. Likewise, her wish to escape only heightened Ali’s anxieties. Mrs. B. felt that she had no friends to talk to and relied totally on her husband. I was becoming aware how Ali’s problems mirrored mother’s internal world. Mrs. B. felt depleted by Ali. She desperately wanted a close friend but had no energy to meet people. She reflected with me about how she was outgoing and had many friends as a child. She felt that she was like the child on the playground who nobody wanted to play with. As Ali progressed, I was aware how Mrs. B. was becoming increasingly more depressed, isolating herself more and more, just like Ali. We talked about Mrs. B. getting help for herself which she was able to do. As she began seeing a therapist and felt a bit better, Mr. B. began talking with me how he had been enduring the emotional burden of supporting his wife and how he, too, needed a break.
The struggle for me as a therapist during this early stage of treatment was the difficulties the parents had in engaging with their child in a nurturing and loving way. Instead, they pushed her away when she approached them, feeling suffocated by their own child, and wishing to escape from her. They felt like they were held hostage by their own daughter. They never experienced what other parents of toddlers could do, the opportunity to observe their child moving away to master the world. As a result, there was a lack of differentiation between parent and child. Ali developed an overdependence on her parents, and as we explored what this meant for Mrs. B., it became apparent how Ali reflected mother’s internal object relations. Mother and child were merged in an anxious and disorganized attachment pattern. For Mrs. B., her child seemed to mirror an aspect of herself that caused her great pain. When she looked at her child and saw that she was imperfect, she reflected that others saw her as an incompetent mother. Mother and child were merged as one but in a position of distress and narcissistic injury rather than a warm and loving attachment to one another.
From the child’s standpoint, Ali was a child who was clingy and viewed the world as unsafe and unpredictable. She was unable to move away and separate from her parents or explore the object and person world because of extreme tactile, auditory, and movement sensitivities and motor planning difficulties. She watched the world and viewed it as a scary place which only fueled her anxieties. She didn’t know how to engage in pleasurable interactions with her parents and other children, and instead, kept her parents close to her to organize and calm her. Her needs were that of a very young infant, not a child of 2 years.
11.4. The school-aged years
When Ali was 6 years of age, she began participating in a social skills group with two other girls. There was a burst in her social skills as a result of the group. She wanted play dates for the first time and seemed to crave time with peers. She went up to people’s houses in the neighborhood and knocked on their doors to ask to play for the first time. She was no longer hanging by her mother’s side—a great relief to her mother. Mrs. B. began to realize how immature Ali was in comparison to peers. They went to the swimming pool and Ali joined in the fun with the other children, but her play quickly became rambunctious, jumping, splashing, and screaming in the water. Other mothers expressed how it must be nice not to have Ali by Mrs. B’s side, but Mrs. B. felt that they noticed how bad off she was. When I saw Mrs. B. for a parent guidance session, she cried, expressing how much pain she felt about Ali’s problems, how she felt paralyzed and depressed by them. I supported her in her feelings and pointed out that she hadn’t had the typical parenting experiences that most parents had, for example, validation by other mothers that she was doing the right thing, feeling ostracized that she had an unusual child, and not having the experience of sitting with other moms and talking while her child ran off to play with other children. We talked about how Mrs. B. felt that it was as if she had no sense of self, that she was always constrained by Ali. I praised Mrs. B. in her efforts with Ali—that it was because of what she had done that Ali was doing the things she was doing now.
Despite the lovely changes in Ali’s social behaviors, her behavior at home became increasingly worse. She was becoming more rude to her parents and doing outlandish behaviors to express her anger at them. She smeared feces all over the bathroom and yelled that she was angry. She said rude things to her parents, then when reprimanded, she would mock them back—“Well, you’re being rude!” When her parents tried time out with her, she would have a huge tantrum. Both parents felt that none of the limit setting worked and felt that 90% of their interactions with Ali were negative. This surge of oppositional behaviors coincided with her increase in social skills. It seemed that Ali’s oppositional behaviors were related in part to the fact that she never learned to negotiate the task of intimacy and engagement, and when she did finally learn to separate, it was with extreme anxiety. Instead, when she engaged with others, it centered around distress and anger. Ali did not know how to assert herself in positive ways. She seemed to be operating at two ends of the continuum—moving from a clingy, fearful child to intense, negative engagement.
During this period, it became more apparent the difficulty that Ali felt in self-calming. She often sought high intensity when engaged with anyone, not just her parents. She would say things like “I just want to be wild,” “I can’t stop myself.” In individual treatment sessions with me, she often submerged herself in the bubble ball bath inside my pup tent, screaming and laughing almost hysterically, wanting me to watch her as she did this. Often she would talk to the balls as if they were real, after which she would seem amazingly calm. In the pup tent she would exclaim things like “Stop, don’t do that!” to the balls.
Ali entered first grade that year in a specialized setting for children with learning and emotional problems. Over this year, we saw how she became overwhelmed with task or situational demands. Her response to requests to do things usually resulted in her becoming defensive, anxious, or avoidant. If she felt she couldn’t do something, she could become bossy or rude. She tried to control the activity by changing the rules to do it her way, or insisting that she could do it even when she couldn’t. We tried to encourage non-competitive activities to give her success in trying new things. I found that what worked well was structuring activities or selecting medium that allowed her to have varying levels of competence from simple to complex (e.g., art, dramatic play, construction toys). Once Ali organized herself, she often took cues from others to modify her responses or to model after them. If I gave too much direction early on, she would balk or becomes anxious. Finding ways to help her to take instruction from others was a major goal as she entered first grade.
Part of my work with Ali at this stage included consultation to her classroom teacher and the occupational therapist at school. I encouraged her teachers and therapist to have a familiar adult help her during transitions in activities, particularly when she had to go into a new situation or be with unfamiliar children. Unstructured activities were very difficult for Ali because of her dyspraxia, word finding difficulties, problems with visual–spatial perception, reading social cues, and executive functioning. For example, it was very difficult for her to walk down the hall on the way to the classroom or the lunch room. Open-ended situations like free play, recess, or field trips were very stressful for her. She wasn’t sure what to do or say. In these situations, she was apt to become a passive observer, show her distress by comforting herself (e.g., sucking on a finger), or by becoming silly (e.g., pretending to be a roaring monster). I suggested to her teachers to give her little assignments during these more open-ended times. For example, when walking down the hall to an activity, they asked her to carry something to be a helper. In large, noisy gatherings, such as the lunch room, we had her sit by the wall at a small table with only a few children, then had her leave the lunch room to a quiet space.
In the individual therapy, I focused on how to problem solve and sequence her thoughts. Ali needed help with being organized and figuring out how to do things on her own. We worked on how to connect ideas logically in a sequence, in understanding the link between actions and consequences, and to evaluate her behavior when problems arose. When we talked about problem situations, she had good skills in thinking through a solution, but enacting the solution in the midst of the problem was difficult for Ali, particularly because she tended to become loud, silly, overstimulated, or disorganized. What seemed to work best was enacting problems through dramatic play and presenting her with problem situations to solve, or prompting her to stop and think through what to do next as she worked through the sequence. I also used visual aids, such as pictures or writing down the steps in a sequence as I helped her to figure out the best way to approach the task, thus playing to her strengths as well. She did well when given a specific verbal script or series of pictures to guide her in taking action. I used videotaping and comic script formats as additional mediums.
The playground was very challenging for Ali. She would usually stand back quietly and watch the other children. By the time she figured out how to enter their play, the children often had moved onto something else. Many times other children didn’t invite her into their play because of this. It helped Ali to be paired with other classmates for projects, allowing her to get to know them in more structured activities. She also did well when cued on the playground of how to get started in play. She responded very well to a behavioral program that we did during that year—the playground program. This program first rewarded her for simply getting out of the car and watching the other children, then rewarding her for standing next to the equipment, and gradually working towards going on equipment without other children nearby to ones with children on it. Moving freely between pieces of equipment on the playground was hard for her, so giving her a sequence of what to do helped. The playground program also focused on her building connections with her mother, using walkie talkies where she could keep a connection with mom at the playground. For example, I suggested that when they used them, mom could ask her things like “See if there are any pine cones under the tree” or “count the number of children you see with white shoes on and report back to me.” We played race cars and remote control airplanes that Ali could move across the field. In her neighborhood, we had Ali deliver flyers to house doors for the county council on a regular basis. We gave Ali a map of the neighborhood and had her do neighborhood watch activities—count number of pink houses, number of green cars, number of barking dogs, and record it in her notebook. We did a similar program around walking into school by herself, having mom first walk her to the front door, then up to the big bush midway up the walk, and eventually having her walk by herself from the drop-off car lane. I also suggested that Ali be given something to carry when they were walking together outside, holding hands only in the parking lot or when crossing a street.
I tried to make the treatment as naturalistic as possible for Ali, we visited Pizza Hut one time to work on her hypersensitivities and fears of noise in this type of setting. Walking up to the trash can was scary for her to throw her trash away or going into the bathroom because of the automatic toilets. We talked ahead about what would happen that she would order pizza, sit with me in the booth, then we’d throw our trash away, and go to the bathroom. With each juncture, she exclaimed to me “I did it,” “I can do it.”
Ali seemed to enjoy school and showed a strong desire to learn, but would become easily upset when she made mistakes. She would say things like “I’m angry” when she couldn’t figure out how to do something. She seemed to do best if she saw another child solving the problem so that she could model after them. This worked better than if suggestions were made to help her. She was very responsive in my group if paired with a verbal child who could provide her with ideas. It didn’t work to focus on her statements of why she was angry. I found that giving her time and space to reorganize calmed her more and my ignoring these comments. She would generally come around within a few minutes, but if I joined her around her statements of anger, she would escalate quickly. Following these outbursts, I would simplify the activity and get her redirected in a productive activity like an art project or play scenario. I often suggested to Mr. and Mrs. B. to try this strategy, but they claimed it never worked for them.
Despite the good progress that I was seeing in Ali, I was struck by how Mrs. B. needed to hear over and over again what was going right for Ali. She seemed not to believe me when I told her how Ali was doing well in group and individual therapy. When I gave her concrete examples, that is, how Ali showed wonderful insight and empathy toward the other girls in the group when she was calm, she wouldn’t believe me and wanted me to say more. Throughout this year, there were some sessions with Mr. and Mrs. B. that they felt completely demoralized, saying—what was the point, nothing worked, and no one understood. I told them that it was Ok to be disappointed and angry with me that I hadn’t been able to make a big enough difference. Some of the ideas I offered to them may have been too difficult or not possible for them to do. I reiterated that I would stick by them and would not abandon them. Their anger at professionals, including me, had been mounting. They were frustrated that no one understood Ali and what her problems were. They were disappointed that professionals had not been successful in making a enough change in their daughter and that no one was addressing the real problem. Mr. and Mrs. B. did not want to acknowledge that Ali might be reflecting the anger of the household and needed to displace it to me and other professionals.
11.5. Ali at 10 years
As Ali turned 10 years of age, we continued in both individual and group psychotherapy. Play themes centered around mastering separation and autonomy but doing so in the absence of an attachment figure. For several years in therapy, Ali had a preoccupation with playing the part of toddlers, selecting dolls that a much younger child might choose. Interestingly, she was terrified of toddlers as a young child, fearful of their noise, boisterous play, and worrying that they might bump into her. I viewed her identification with the toddler as a need to master her early fear and to enact a stage of development that she never experienced. She would select Barbies for the parents and picked little dolls for the toddlers. She designated me to be the less able toddler who was a few months younger than her doll’s age. My role was to admire her doll’s competence and robust and daring nature. A typical play scenario would be that her doll would become very excited about packing up to go on a vacation. She would call my doll to invite me along on the trip. Inevitably, something would happen to the mother doll during the preparation for the trip. Usually the father would accidentally ride his jeep over mother’s long pony tail while she was in the driveway. The mother would scream “I just washed my hair,” then she would take another shower. As she played the various roles out, she spoke in deep voices for the father, and young, child-like voices for her doll, wanting me to assume similar kinds of voices. The family would load up and go to a vacation spot out on a desert island. In the play, my doll would meet her family on the desert island. The parents would settle themselves in chaise lounges on the beach and the two of us would go do something dangerous in the ocean waters. Usually we took a row boat out into shark infested waters or we would become accosted by pirates at sea. If I expressed anxieties, such as “Are you sure this is a good idea? I’m really scared of sharks”. S would respond, “Don’t worry. I’ll protect you”.
In several episodes of this story, our dolls were taken hostage by pirates and thrown into the dungeon inside the ship or thrown into a dark cave in some remote secluded place. Her doll always escaped and ran for help while my doll remained helpless and scared. In the end, her doll would save me from the dark dungeon by fighting off the pirates. Throughout the episode, the parents didn’t notice the children’s disappearance and were unconcerned for their safety. Ali seemed relieved for me to experience and understand what she had been struggling with for years, her fear of the outside world, lack of protection, and abandonment.
Over the years in my work with Ali, she often carried transitional objects as a way of comforting herself when out and about in the world. As a toddler, her comforting objects were a lemon, a bicycle helmet, and a paint roller and tray, all odd and hard objects, certainly not very cuddly. In the school years she latched onto Weazer, a doll she found at a yard sale that was very dysmorphic and reminiscent of the objects in Toy Story. Its hair was cut off and what was left was dyed pink. There was a light bulb on the scalp; metal bars jutting out for shoulders, and a hideous looking face. She brought Weazer with her everywhere and to her therapy sessions. Often Weazer was integrated into our play, and frequently I was cast in the role of Weazer’s mother. Could I love this distorted doll?
By the time Ali was 10 years old, she began carrying a large stuffed black labrador retriever with her, something that persisted for several years. It looked quite odd to see this dog on a young adolescent’s lap in the waiting room, so I asked her to bring the dog in a back pack so that it would look more socially appropriate.
11.6. The teen years: containing dangerous impulses while creating meaningful attachments
As Ali grew into her teen years, she continued to play with dolls like a much younger child, but the play evolved into the use of paper dolls that she made from magazine pictures of rap singers. She spent long hours in her bedroom at home playing with her paper dolls. Her mother reported that when she listened at Ali’s door, she could hear a lot of street talk and vulgar language. When I asked Ali why she liked rap singers, she replied that she loved their gestures, clothing, and street talk. Sometimes in her work with me, Ali liked doing role plays using dress-ups. They were quite funny and engaging. The vignettes were of people in different situations, such as an ex-beauty queen riding on a bus with a broken heel. She spoke in different voices with accents to accommodate each character, ad-libbing her dialog with me. I found it interesting that Ali enjoyed mimicking different kinds of voices, particularly deep male voices. I viewed the role playing as a way of helping Ali understand how people act, feel, and think. It was highly interactive and emotionally motivating for her.
By the time Ali was 16 years old, her play with the paper dolls stopped, but she became interested in writing stories at home. They were long plot-less stories about rap stars containing vulgar language. Her mother was deeply troubled by this, but I suggested that she allow her to write for a short period each day (i.e., 30 minutes) to give her an outlet for tension release. Ali reported to me that she “had to do this” and if she didn’t, she felt enormously stressed.
Ali had no friends until she reached high school. She attended a private school for students with learning disabilities and eventually developed a few superficial friendships with the kids in her class. Until that time, her only social relationships were with her family members and me. She seemed to have no desire for friends. In her interactions with me, she remained physically stiff and awkward, walking and moving like a robot. Her eye gaze was odd, looking askance and not scanning to look at my face or others’ emotional displays for feedback. In the social skills group that she participated in for many years, she sat there stiffly, not initiating any conversation unless prompted by questions. In contrast, when I saw Ali before the group in individual therapy, she would be quite spontaneous and relaxed with me, but as soon as we walked into the waiting room or group therapy room, she froze up. It seemed that the stimulation of more than one person in the room was overwhelming to her. I wondered how much her inefficient visual scanning and tactile defensiveness put her physically on guard and resulted in a shut-down state.
When Ali turned 18, she went to community college as an art student. Over the next few years, I saw Ali intermittently, usually around incidents when she had done something very impulsive. On one of these occasions, she decided to cut all her hair off. When she came down to breakfast in the morning, her parents were shocked to see her hair hacked off and later found the hair strewn about in the bathroom sink. Mrs. B. was extremely upset and felt that once again, here was another reminder of Ali’s poor judgment and manifestation of her distorted body image. I reframed the incident for her, suggesting that Ali didn’t know how to assert that she wanted to have a new hair style. They took her to a hair salon and reshaped the hair, but it was in such bad shape that they had to get a wig for her to wear. Surprisingly, Ali liked the wig stating that it felt good on her head.
Other incidents of this sort happened in the upcoming years, but despite this long journey, Ali was able to leave for college in her junior year, live on-campus, and make friends with the girls on her dorm floor. She had become serious about studying art and liked living independently. From time to time, she calls me to let me know how she is doing. In one of our recent sessions, she said to me, “You know who you are to me. You’re like a second mom.” How lucky I was to know her.
12. Summary
Sensory integrative disorders involve a dysfunction in the child’s capacity to modulate incoming sensory input to allow for purposeful adaptation to the environment. These disorders are common among learning disabled and emotionally disturbed children and may be observed as early as infancy. The tactile system is important for protection and survival and impacts motor and reflex development, tactile perception, motor planning, and emotional stability. The tactile dysfunctions most commonly observed are tactile defensiveness and tactile hyposensitivities. Tactile defensiveness is a severe sensitivity to being touched that may be environmental, other-initiated, or self-initiated. On the other hand, children with tactile hyposensitivities do not experience touch unless it is very intense.
The vestibular system impacts development of body posture, muscle tone, ocular-motor control, reflex integration, and equilibrium reactions. The vestibular system is important in motor planning, arousal and alertness, and security when moving in space. The common vestibular-based problems include gravitational insecurity, under-responsiveness to movement in space, intolerance for movement, postural-ocular movement disorder, vestibular-postural deficits, bilateral integration and sequencing problems, and dyspraxia.
Developmental dyspraxia is a disorder in the planning and direction of goal-directed movements that are skilled or nonhabitual in nature. Motor planning problems are typically based in the somatosensory and vestibular systems and affect postural movements, sequencing movements, language, spatial constructions, drawing, and symbolic use of objects.
In addition to describing the different types of sensory integrative dysfunction and common symptoms observed during infancy through childhood, this chapter presented treatment strategies for children with sensory integrative dysfunction in infants and children.
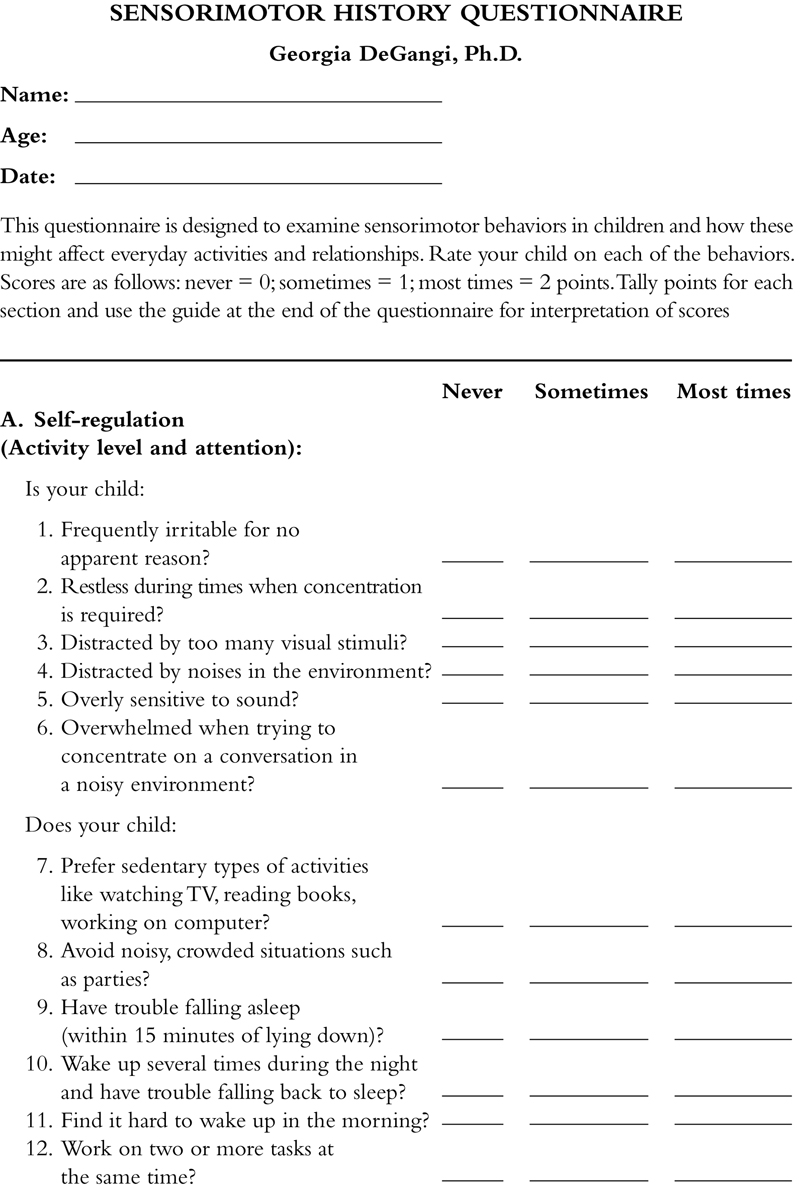
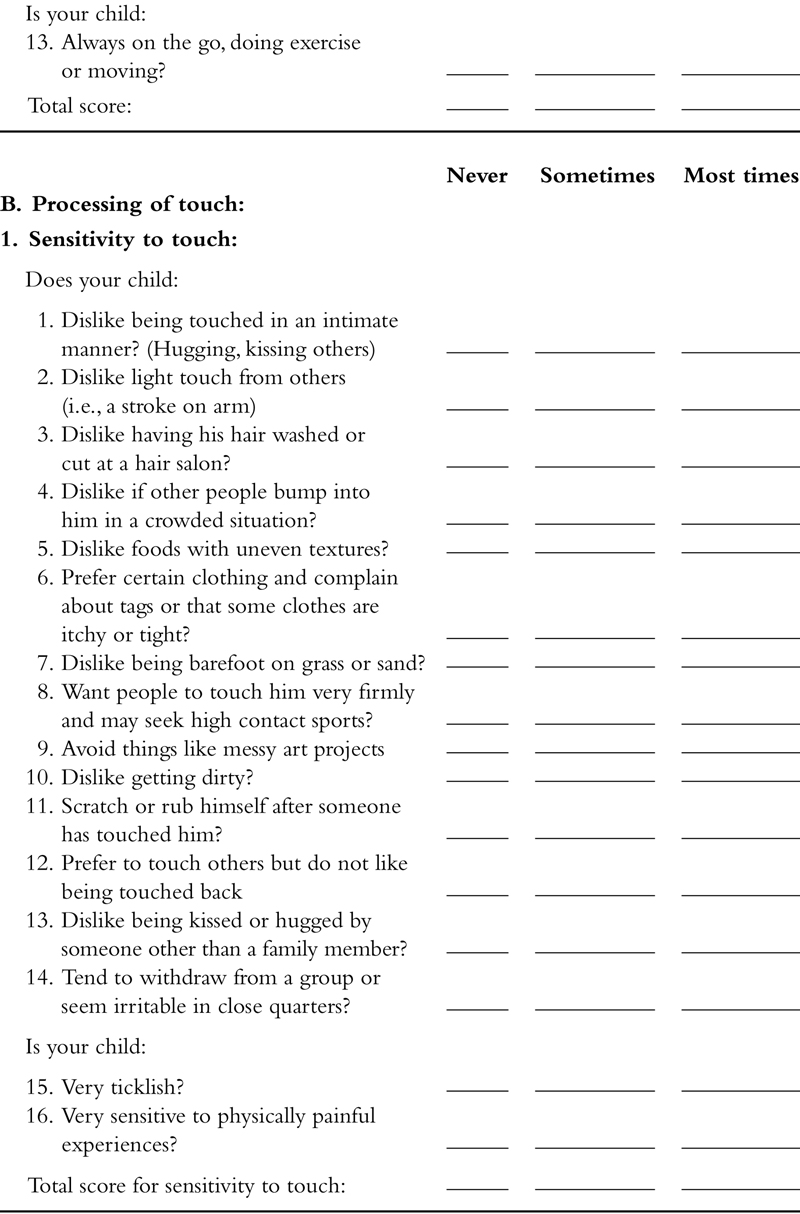
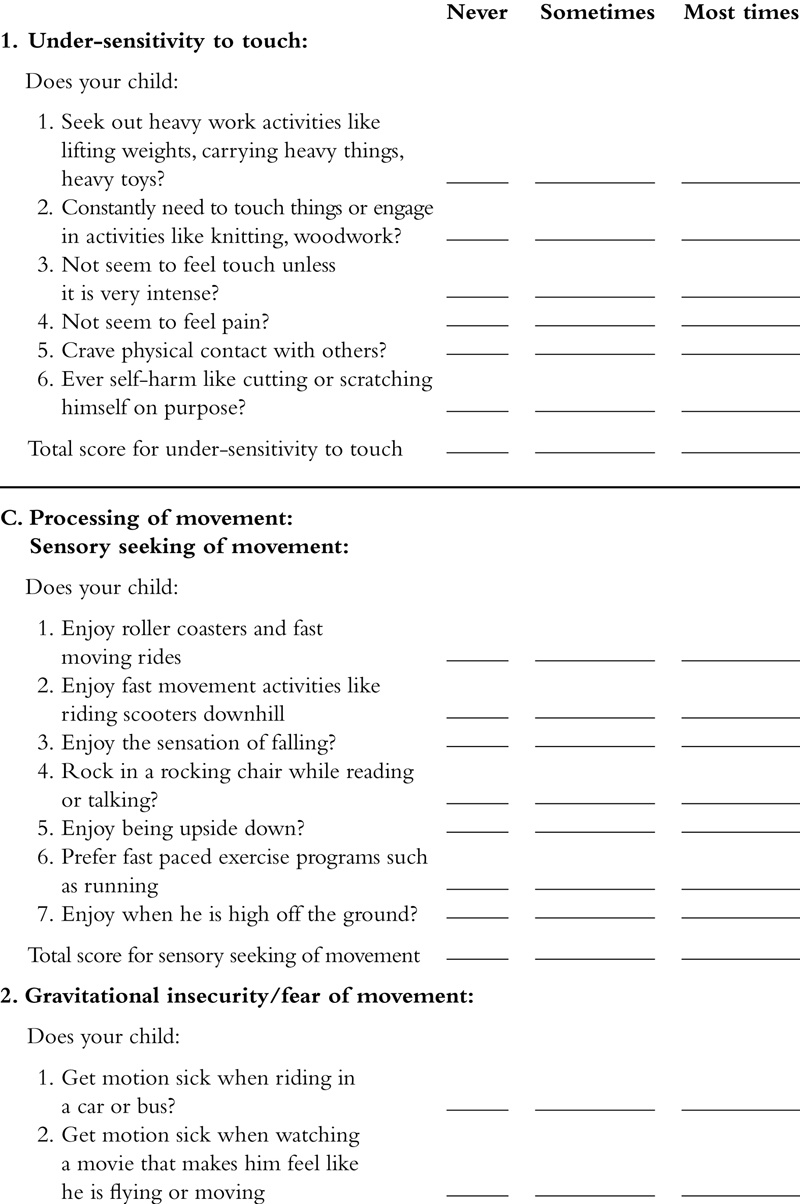
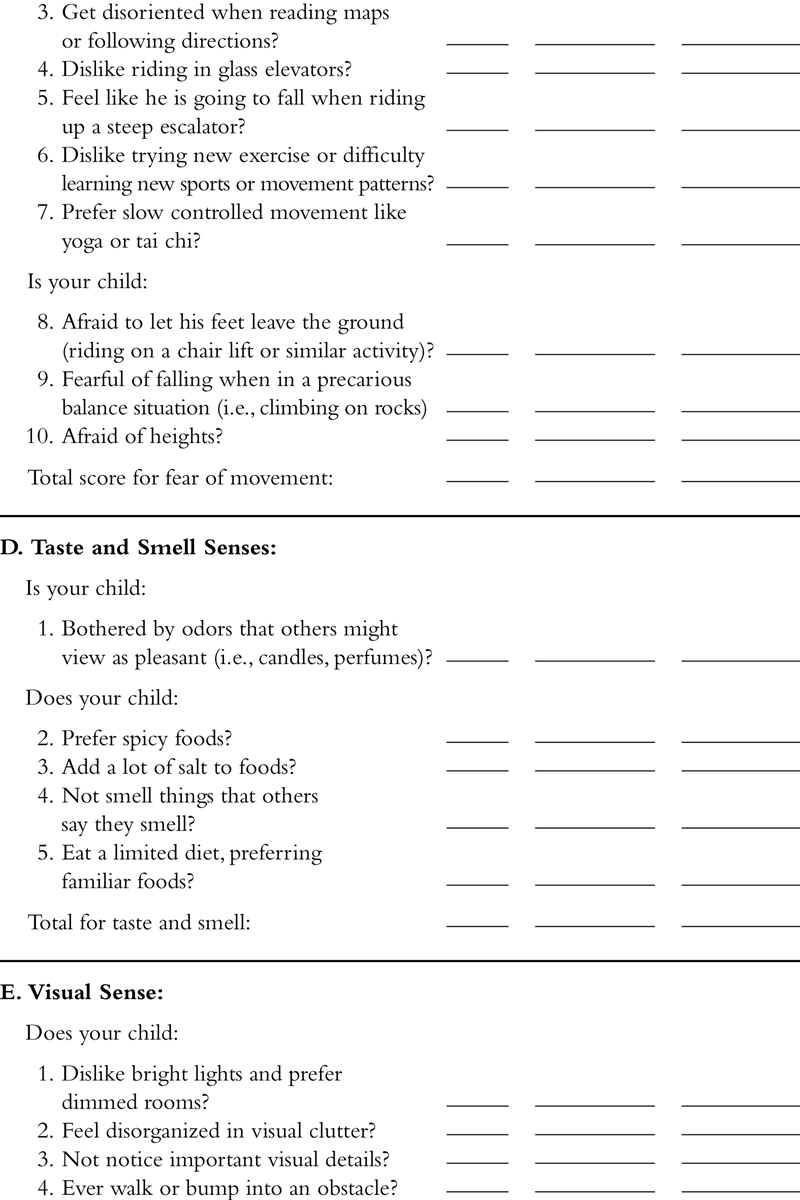
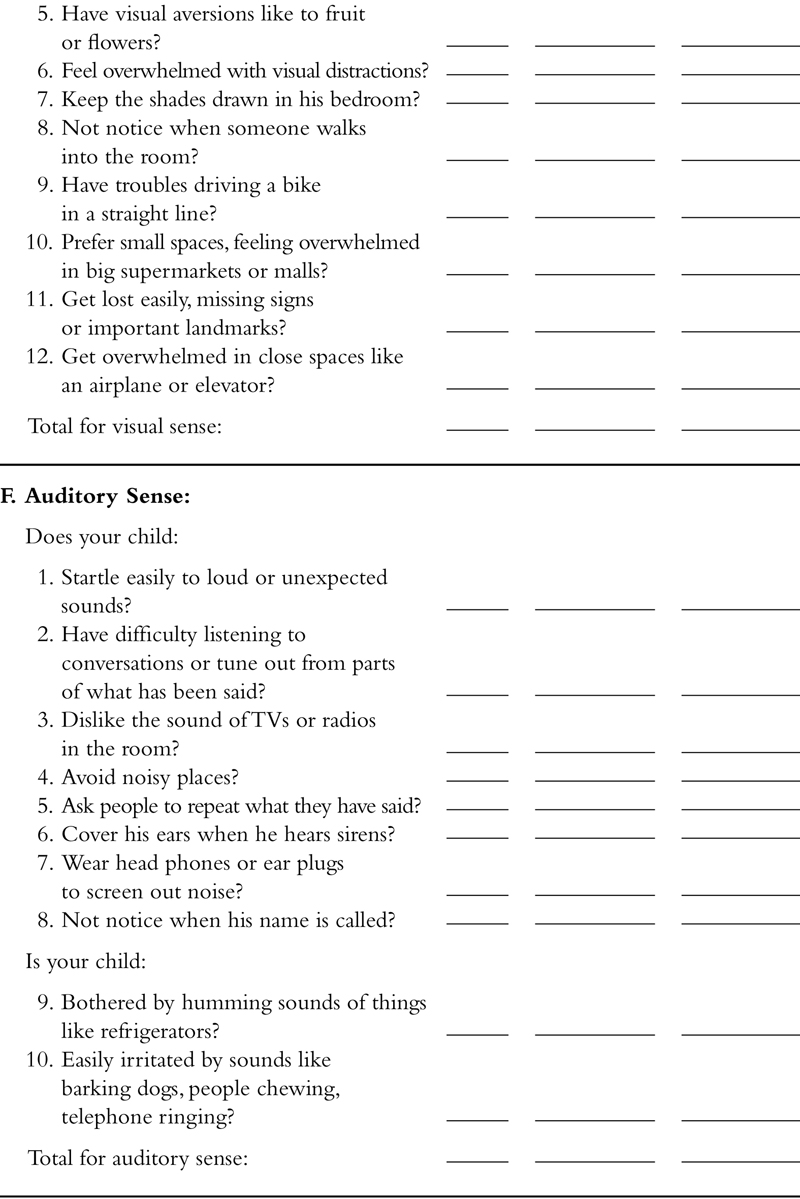

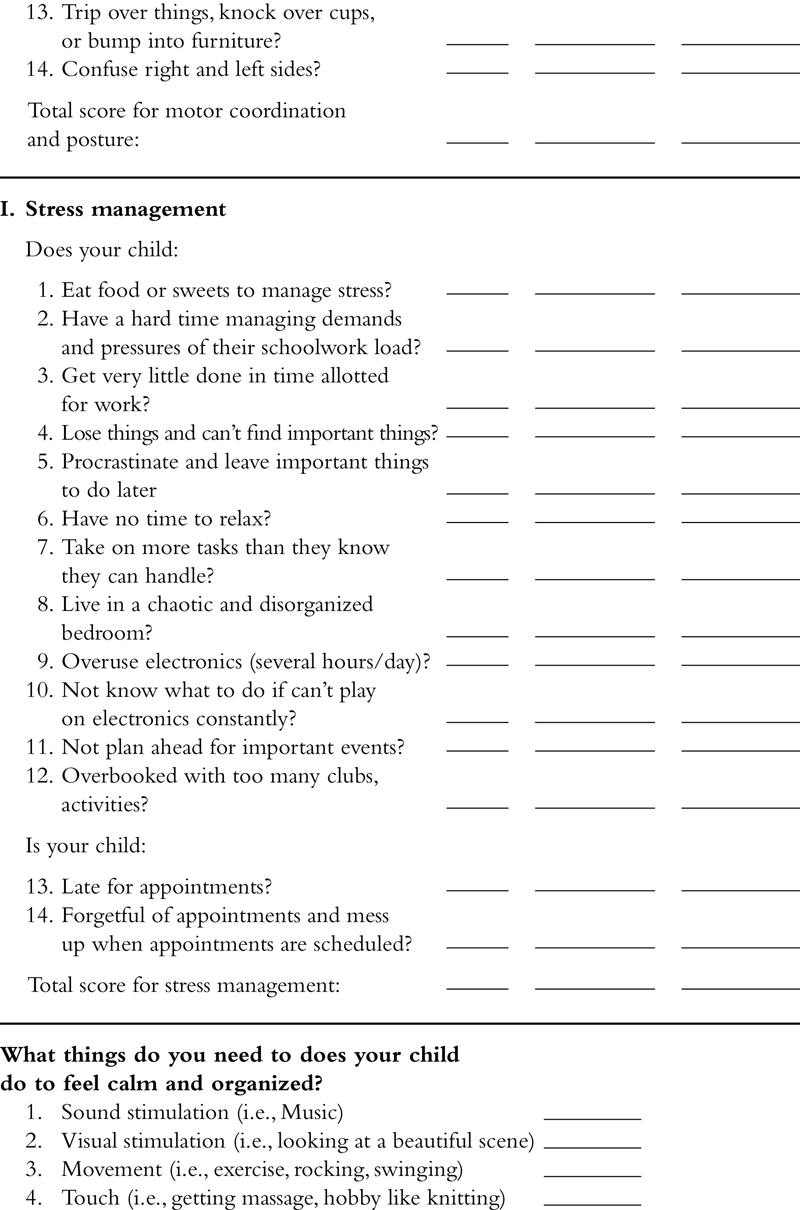

..................Content has been hidden....................
You can't read the all page of ebook, please click here login for view all page.