CHAPTER 4
America’s Self-Created Opioid Tragedy
The saga of America’s opioid crisis reads like The Godfather, except that organized crime never caused this level of chaos, community devastation, and death. The Healthcare Industrial Complex (the System) created and turbocharged the opioid crisis on an unsuspecting public. Nefarious collaboration between Congress, industry, and government agencies makes the System complicit in dealing dangerous drugs to vulnerable populations for gargantuan profits.
The opioid epidemic is devastating communities across the country. The human toll is catastrophic. In September 2017, the Cincinnati Enquirer released “Seven Days of Heroin: This Is What an Epidemic Looks Like,” which chronicles an ordinary week of addiction misery in metro Cincinnati.1 In their investigative report, more than 60 Enquirer reporters, photographers, and videographers bring to life the heartbreaking stories of a region ravaged by opioid addiction. The one-week statistics are breathtaking, gruesome, and mind-numbing:
• 18 deaths
• 180+ overdoses
• 200+ heroin incarcerations
• 15 heroin-addicted babies born
Crony capitalism created and sustains the opioid crisis. A predatory drug company designed an addictive painkiller, then marketed it heavily. Government regulators failed to guarantee the drugs’ safety and efficacy. Doctors accepted gifts and payments that encouraged excessive prescribing. Distributors and pharmacy benefit managers (PBMs) fulfilled massive orders to suspect clinics and pharmacies. Pharmacists filled prescriptions with high-probability knowledge that they would be resold or abused. As a result, millions of patients became addicted to drugs they believed would heal them. Hundreds of thousands have died from overdoses.
Opioid use has spread addiction far beyond patients. Opioid-related addiction, crime, social service needs, human suffering, and loss of life have devastated families and communities throughout America, particularly in rural areas.2 The Healthcare Industrial Complex (aka the “System”) has unleashed a modern plague upon an unsuspecting American public.
AMERICA’S NEW ADDICTION
The sudden death of superstar musician Prince in April 2016 gave a face to a growing American tragedy. Prince’s life was remarkable; his death was not.
Playing all his own instruments, Prince beguiled fans for almost 40 years and had 13 Top 10 songs. His unique musicology combined soul, funk, gospel, and rock genres. Still going strong at age 57, Prince succumbed to an overdose of fentanyl, an opioid commonly prescribed for chronic pain. Fentanyl is up to 50 times more powerful than heroin.3
Opioids are synthetic derivatives of heroin. They are highly addictive. Nearly 4,000 people become addicted to opioids every day. Almost 1,000 of those opioid addicts, 23 percent, also become heroin addicts.4
According to the US Surgeon General, 78 people die from opioid overdoses every day.5 The mounting death toll from opioid overdoses is horrific (Figure 4.1).6 In 2016 alone, 42,259 people died from overdosing on opioids according to the CDC. This represented two-thirds of all drug overdose deaths.7
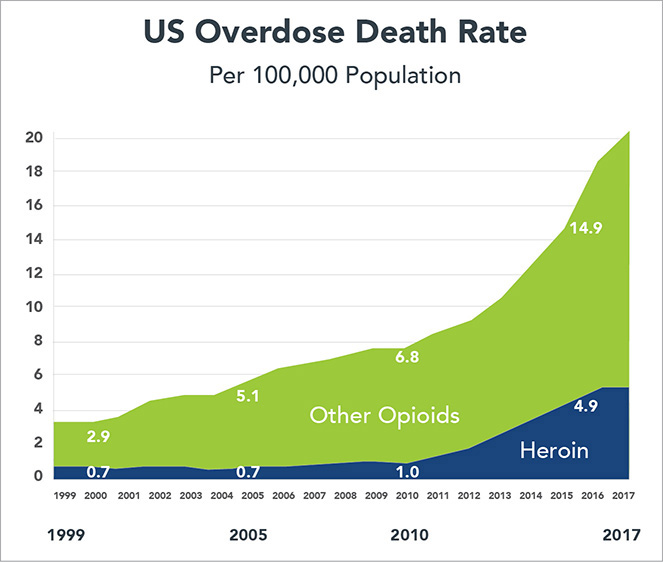
FIGURE 4.1 Skyrocketing opioid and heroin overdose deaths go together like crime and punishment. Between 1999 and 2010 most of the increase in opioid overdose deaths was from synthetic opioids, not heroin.
Despite this all-too-common tragedy, opioids are still mainstream American medicine. Pharmaceutical companies develop and market opioids. The US Food and Drug Administration approves and regulates them. Physicians prescribe opioids abundantly to football players, military veterans, cancer patients, and others suffering from chronic pain.
Support in the American medical community is a principal reason the United States prescribes far more opioids for pain relief than any other country—for example six times more than France. Moreover, the United States accounts for 99 percent of the powerful and highly addictive hydrocodone (better known by brand names Vicodin, Norco, Lorcet, etc.).8 The opioid crisis is a uniquely American creation. Opioids are nondiscriminatory in devastating lives and communities. Addicts cut across societal ranks—rich, middle class, and poor. Opioid abuse and addiction inflate healthcare costs, increase criminal activity, and overburden social services.
ILLICIT ORIGINS
Early studies suggested that opioid painkillers were not addictive. In the mid-1990s, the American Pain Society emerged and embraced these findings. They stressed the need to treat pain as the fifth vital sign (along with temperature, pulse, blood pressure, and breathing rate) even though clinicians cannot measure it with precision. As the new millennium arrived, the Joint Commission for Hospital Accreditation, the Veterans Administration, and other medical organizations stressed the need to manage pain more aggressively.9 Medical training promoted pain management with opiates as a best practice, driven in part by aggressive pharma-funded “education” programs that often included all-expenses-paid conferences at plush resorts.10
Until OxyContin came to market in 1996, doctors prescribed opioids in limited fashion to manage severe pain associated with serious injury or illnesses. OxyContin is a formulation of oxycodone developed by Purdue Pharma, a privately held pharmaceutical company based in Stamford, Connecticut. OxyContin offered longer-lasting pain relief—up to 12 hours per pill. Prior to Oxy, patients took pain pills, such as Percocet, every four to six hours. Marketed by Purdue as a miracle drug, patients and physicians hopped on board the Oxy Express. Today, OxyContin is America’s bestselling painkiller. Purdue Pharma has aggressively marketed the drug and reportedly achieved $35 billion in sales from 1997 to 2016.11
In reality, OxyContin’s pain relief does not last 12 hours. Pain returns earlier than expected. Patients crave relief.12 By continually dosing, many deplete their supply prematurely. They ask physicians for more drugs until refused. They hide their addiction, seek drugs elsewhere, and lose control of their lives.
In 2007, Purdue Pharma pled guilty to criminal charges that it misled doctors, regulators, and patients about OxyContin’s potential for abuse. The company paid $600 million in fines and legal fees. Purdue’s president, medical director, and top lawyer pled guilty to related fraud charges and paid a $34.5 million fine.13
Purdue is not alone in conducting questionable and/or illegal opioid marketing. The FBI arrested INSYS Therapeutics executives in December 2015 for bribing doctors and defrauding insurance companies to increase fentanyl sales.14
While awareness of the dangers of abuse and addiction has improved, overprescribing continues to be a major problem. Each year, doctors prescribe the equivalent of one bottle of opioids for every American.15 Patients with temporary postsurgical pain typically receive 30-pill prescriptions when 3 or 4 pills would suffice.
Deadly addictive opioids fill the nation’s medicine cabinets as a result, and these drugs are difficult to track and control. Opioid addiction usually starts when individuals experiment with painkilling drugs prescribed for themselves or someone they know. Big Pharma provides that initial fix and feeds the addiction by flooding American communities with oxycodone, hydrocodone, fentanyl, and other opioid-based drugs. Most opioid addicts get their first pills from relatives and friends versus doctors. Excessive prescribing has created a black market for resale of surplus opioids. Addicts buy opioids when they can. Many switch to less-expensive heroin when they can no longer afford or acquire prescription painkillers.
A December 2016 article in the Charleston Gazette-Mail reported that drug distributors delivered 780 million oxycodone and hydrocodone pills to West Virginia pharmacies between 2007 and 2012.16 That translates into 433 opioid pills for every man, woman, and child in the state. During that period, 1,728 West Virginians died from overdosing on those drugs.
In a 2016 report, the US Surgeon General stressed that substance abuse and addiction are symptoms of chronic illness:17
For far too long, too many in our country have viewed addiction as a moral failing. This unfortunate stigma has created an added burden of shame that has made people with substance use disorders less likely to come forward and seek help.
It has also made it more challenging to marshal the necessary investments in prevention and treatment. We must help everyone see that addiction is not a character flaw—it is a chronic illness that we must approach with the same skill and compassion with which we approach heart disease, diabetes, and cancer.
It wasn’t enough for the System that opioids were killing Americans at alarming numbers, particularly in rural areas. When the DEA undertook an aggressive campaign to close down overprescribing pharmacies or “pill mills,” Big Pharma and their friends in Congress and government used their clout to curtail the DEA’s enforcement efforts. This case study illustrates how the Healthcare Industrial Complex plies its trade.
BIG PHARMA SQUELCHES THE DRUG ENFORCEMENT ADMINISTRATION (DEA)
Talk about bombshells. On October 15, 2017, the Washington Post and 60 Minutes released a detailed and damning investigative report titled “The Drug Industry’s Triumph Over the DEA.”18 The report chronicles how Big Pharma and its congressional allies orchestrated passage of legislation that has severely weakened the DEA’s ability to curtail illegal distribution of opioid drugs. Here’s what happened.
The Drug Enforcement Administration (DEA) intensified its investigation of drug distribution companies in 2006 as the opioid epidemic was worsening. An aggressive enforcement effort led by Joseph Rannazzisi (investigation) and Linden Barber (litigation) began targeting wholesale drug distributors servicing “pill mills.” The “big three,” McKesson, Cardinal Health, and AmerisourceBergen, distribute 85 percent of the nation’s drugs.
Under the 1970 Controlled Substances Act, distributors have a legal and ethical obligation to report suspicious opioid deliveries. The DEA had two enforcement mechanisms for stopping suspicious sales: (1) issue an “order to show cause” that gives companies 30 days to respond to allegations of wrongdoing; and (2) issue an “immediate suspension order” where the DEA immediately halts commerce from that company in targeted substances.
Many Big Pharma companies, including the big three mentioned above, have paid large fines for improper opioid distribution. These fines represent a small percentage of the billions of dollars earned by pharmaceutical companies selling, distributing, and dispensing opioids. For the record, the Drug Enforcement Administration collected $425 million in fines over a 10-year period beginning around 2006.19
Even though the fines were a relative pittance, Big Pharma objected to the DEA’s aggressive enforcement approach and fought back. Collectively, the pharmaceutical industry hired 56 former DEA and Justice Department officials, including Linden Barber, to execute their attack on the DEA. Their goal was to limit the DEA’s stepped-up enforcement against drug distribution companies.
Big Pharma lobbyists worked behind the scenes with select members of Congress to draft legislation to curtail the DEA’s enforcement powers. Money talks. Between 2014 and the law’s 2016 passage, Big Pharma spent $106 million lobbying for the Drug Enforcement Act. Barber testified as an expert witness, explaining why the new legislation was necessary. His testimony had an Orwellian ring to it:
As a supporter of DEA’s mission, I urge the committee to take legislative action that clarifies the definition of imminent danger.
Barber’s statement is reminiscent of the Vietnam-era Pentagon press quote that “it became necessary to destroy the town (Ben Tre) to save it.”20 With Big Pharma’s drafting help, Congress “clarified” the definition of “imminent danger” to an extent that made Drug Enforcement Administration’s use of imminent suspense orders almost impossible to justify.
Starting in 2015, new leadership at the DEA (Chuck Rosenberg) and the Justice Department (Loretta Lynch) committed to “working more closely” with the pharmaceutical industry. Reflecting the new, more cooperative approach, Lynch’s office informed Congressman Tom Marino that the DEA had met with 300 pharmaceutical industry representatives since she had taken the helm at Justice. By contrast, Lynch’s predecessor (Eric Holder) took the unusual step of publicly opposing the Drug Enforcement Act.
After industry complaints regarding Rannazzisi’s forceful investigative style, the Drug Enforcement Administration relieved him of managerial responsibility for its 600-person investigative unit and began an internal investigation. In response, Rannazzisi retired in 2015 after a 30-year career with the DEA.
For several years in a row, Pennsylvania Representative Tom Marino sponsored legislation to weaken the DEA’s enforcement powers. The “2016 Ensuring Patient Access and Effective Drug Enforcement Act” gutted the DEA’s ability to halt questionable sales of prescription pain pills. As a result, the DEA’s number of “immediate suspension orders” against suspect doctors, pharmacies, and drug companies plummeted from 65 in 2011 to just 8 in 2016.
Notice the irony that the “Drug Enforcement Act” actually made it harder for the Drug Enforcement Administration to stop and punish behaviors that fueled the opioid industry—and crisis. It took four tries, but Marino finally passed the 2016 Drug Enforcement Act with unanimous voice votes in the House and Senate. President Obama signed Marino’s bill into law on April 19, 2016.21
Passage of the 2016 Drug Enforcement Act capped a multifaceted, multiyear effort by the pharmaceutical industry to diminish the DEA’s ability to interfere with its commercial interests. The Drug Enforcement Administration and the Justice Department had fought against the legislation for years but ultimately chose to accept it. Big Pharma won. Society lost.
CRONY CAPITALISM ON THE RISE
Reaction to the Washington Post and 60 Minutes report was swift and consequential. Pennsylvania Representative Tom Marino, the principal sponsor of the 2016 Drug Enforcement Act, withdrew his name from consideration for becoming President Trump’s drug czar. Missouri Senator Claire McCaskill immediately introduced legislation to restore the DEA’s ability to execute more aggressive suspension orders.
The 2016 Drug Enforcement Act is what crony capitalism looks like. Powerful industry lobbyists capture the government’s policy-making apparatus to advance their own interests. In 2018, drug manufacturers and pharma supply-chain companies employed more than 1,100 lobbyists—almost two for every member of Congress.22 In 2016, pharma spent almost $100 million more on lobbying than the next highest-spending industry group.23 Big Pharma’s ability to manipulate market supply and demand for dangerous opioid drugs makes an already dire situation worse.
Industry capture of the government’s policy-making apparatus is dangerous to democracy. Big Pharma’s ability to pass the Drug Enforcement Act is a textbook example of a powerful industry hijacking public policy and limiting government’s policing power. Senator McCaskill’s description of the 2016 act’s passage reveals crony capitalism at play in the halls of Congress:
But it’s really insidious in that, you know, these drug distributors hired people out of the DEA, and then they went to work trying to wear down the DEA as it relates to changing this law. Members of Congress who were pressing this law, you know, tried to keep saying, you don’t have a good working relationship with the distributors.
Meanwhile, these distributors were sending 9 million pills into a small community in West Virginia that had fewer than a thousand people. Obviously, they were not trying to do their best job in terms of making sure these products were [not] diverted to the black market. So, I think this was Congress not paying close enough attention, pharma and the drug industry having too much influence and the revolving door that so often helps industries get their way.24
This is the System at work, pushing unneeded and addictive opioid drugs on an unsuspecting and trusting public. Public outcry has driven efforts to reduce opioid prescriptions, address addiction, and increase distribution of lifesaving naloxone, which reverses opioid intoxication or overdose.
Like epinephrine (the drug used in EpiPens), naloxone is a readily available, low-cost, off-patent drug with proven efficacy. Like EpiPen manufacturer Mylan Pharmaceuticals, naloxone manufacturers generate their massive profits by creating easy-to-use (and easy-to-replicate) delivery mechanisms that receive FDA patent protections. The New England Journal of Medicine reports that naloxone manufacturers, not missing a massive profit opportunity, are dramatically raising prices as demand for their products increases (Figure 4.2):
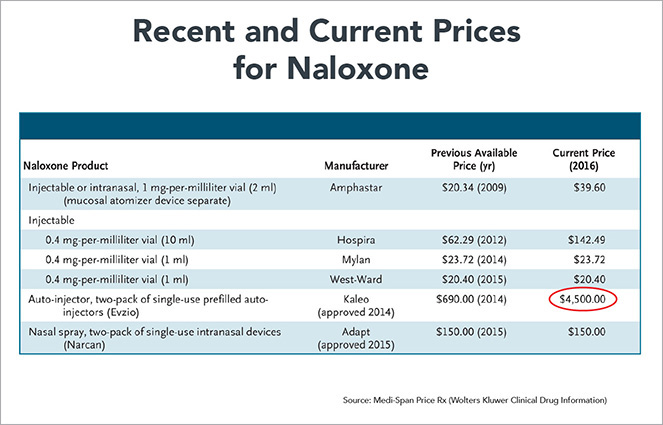
FIGURE 4.2 The price of the two-pack of prefilled auto-injectors, which is most often used with children, has increased sevenfold.
Each formulation of naloxone—two injection doses, Narcan nasal spray, and Evzio auto-injector—essentially has one supplier. Though there are three manufacturers with FDA approval for 0.4-mg-per-milliliter-dose injections, the vast majority are sold by Hospira, which has increased the price by 129% since 2012. . . . Only Amphastar manufactures 1-mg-per-milliliter injections, the dose used off-label as a nasal spray, which currently costs $39.60 after a 95% increase in September 2014. Newer, easier-to-use formulations are even more expensive. Narcan costs $150 for two nasal-spray doses. A two-dose Evzio package was priced at $690 in 2014 but is $4,500 today, a price increase of more than 500% in just over 2 years.25
Unlike naloxone manufacturers, the Mission Health system has resisted the temptation to amplify profits by providing high-cost treatments for opioid addiction. Mission serves the people of largely rural western North Carolina. Twelve percent of the babies born in Mission hospitals are opiate addicted and require detoxification. Detox occurred in expensive neonatal intensive care units (NICUs) until Mission’s physicians developed a more effective, home-based detox program. This procedure is significantly less expensive, it enhances the nascent mother-child relationship, and it also advances childhood development. Each day a baby spends in a NICU requires two days of recovery time with its mother.
For all its great work helping babies, Mission experienced $4 million in lost NICU payments for the less invasive detox treatments. Doing the right thing for mothers and children cost the health system money.
CRONY CAPITALISM HAS CONSEQUENCES
The System has the blood of the American people on its hands. Healthcare’s “iron triangle” worked diligently over a long period to infect American communities with this scourge of opioid addiction. All component parts coordinated to achieve this conclusion:
• Medical researchers didn’t qualify their findings.
• Manufacturers lied about opioid safety and benefits to turbocharge sales.
• The FDA approved products without adequate review.
• Revolving-door professionals shuttled between government and industry, advancing industry interests with insider information and relationships.
• Interest groups spread propaganda on pain management.
• Medical professionals embraced pain as a fifth vital sign and accepted perks for prescribing opioids.
• Drug distributors resented DEA interference in their business operations and worked to eliminate it.
• Medical schools didn’t challenge industry-led protocols.
• Members of Congress took Big Pharma’s money to do their bidding.
This shameful behavior created a public health challenge that will require decades, resources, and funding to address. Ironically, Congressman Tom Marino would be leading this effort as President Trump’s drug czar if the Washington Post and 60 Minutes hadn’t exposed his leading role in limiting the DEA’s enforcement capabilities.
One final note. In November 2018, then FDA Commissioner Dr. Scott Gottlieb (he resigned his position in April 2019) announced that the FDA had approved Dsuvia.26 Dsuvia is an opioid drug manufactured by AcelRx Pharmaceuticals that is 10 times more powerful than fentanyl (the drug that killed Prince). This approval was highly controversial. The FDA granted it despite vocal opposition from four US senators and the FDA advisory panel chair. Opponents worry about Dsuvia’s addictive potential, its easy-to-divert pill delivery mechanism, and its lack of unique medical properties.27
The American people should be afraid, very afraid.