
CHAPTER 2: WHAT EXACTLY IS A PANDEMIC?
Historically, pandemics can be traced back many centuries. A simple definition that has been used to describe them is “a contagion that has gone global”. Although a pandemic can also affect the animal and bird populations, this book focuses on the human-to-human spread of potentially fatal contagions.
The WHO tells us that this worldwide spread of a novel disease will initially have no vaccines or known cures available, and neither will people have any immunity. Generally, the most common cause of pandemics has been influenza, although in the past 75 years, almost 400 new infectious diseases have been discovered. Since 1971, scientists have identified 25 new pathogens for which we have no vaccines and no treatment, although most have not developed into a pandemic (Quick, 2018, p 41).
Influenza in its various viral forms certainly deserves more than just a passing mention in the history of pandemics. Most notable is the 1918-1919 Spanish influenza outbreak, which alone is estimated to have killed more than 50 million. History has taught us that we can expect an average of three influenza pandemics each century.
In the Middle Ages, caused by the Yersinia pestis bacteria, the bubonic plague, or Black Death as it became known, killed close to 20% of the global population. It ran from 1347-1351, and resulted in an estimated 75 million fatalities out of a world population of 450 million. Localised plague outbreaks do still occur in various parts of the world, but they are generally controlled by antibiotics.
One exception is HIV/AIDS, which was identified around 1980 and has killed almost 40 million in the four decades since its discovery. It is estimated that as many people, primarily in sub-Saharan Africa, are also living with the disease. The origin of HIV/AIDS has been traced back to Cameroon in Africa, as early as 1910. The disease had been in existence for around 50 years before it finally exploded onto the global scene. There is still no vaccine or known cure, but it is now treatable by using what is known as antiretroviral medication.
Perhaps also worthy of mention, although maybe not in the same league as the aforementioned pandemic causes, since first spreading from its origin in the Indian sub-continent around 200 years ago, over an extended period cholera has also killed millions. The WHO has estimated an annual case diagnosis of up to five million, with as many as 120,000 associated deaths. Cholera is treatable and a combination of rehydration and antibiotics are usually prescribed. However, if left untreated, cholera can kill in a matter of hours.
“The Covid-19 pandemic has made clear that our health is inextricably tied to larger environmental issues. Increased population density, global travel, deforestation, large-scale farming and melting of the permafrost has disrupted animal habitats, bringing them in closer contact to humans. This has raised the risk of more frequent zoonotic disease outbreaks and therefore a higher potential for another pandemic.”
(Morrin, 2020)
In 2020, the threat from the novel virus subsequently named SARS-CoV-2 appeared. We now know that this causes the potentially fatal disease that was named COVID-19.
Depending upon the nature of a contagion, it can be transmitted from human to human in any one of a number of ways, including:
• Airborne infection – usually caused by organisms that can survive suspended in the air for long periods.
• Droplet infection – occurs usually from the droplets generated by coughing or sneezing.
• Vector-borne – e.g. carried by mosquitoes, fleas, mites, ticks.
• Direct contact infection – can result from skin-to-skin contact or exposure to contaminated body fluids.
• Indirect contact infection – can occur by touching a contaminated surface (e.g. door handles, handrails or elevator call buttons).
2.1 Known diseases that could cause a pandemic
The WHO has listed a number of diseases on its website that it believes have the potential to develop into epidemics and pandemics. Some of those listed already have achieved epidemic or pandemic status, and their names will no doubt be familiar to readers. Our business continuity and pandemic response plans should be prepared and maintained with these in mind.
It is also worth noting that, over time, the WHO will keep that list updated to reflect any emerging infectious diseases, such as COVID-19, as and when they are identified. In the meantime, I have broken these particular threats that we are facing into three sections. Those that are:
1. Capable of causing a global pandemic.
2. Capable of causing devastating regional epidemics.
3. Those that have the potential to be used in the pursuit of biological warfare and bioterrorism, to which section 2.2 has been devoted.
2.1.1 Global pandemic contenders
These include respiratory viruses, such as pandemic influenza, coronaviruses (between 2002-2019 there have been three), Nipah virus and a small number of others, including as yet unidentified emerging infectious diseases.1
2.1.2 Devastating regional epidemic candidates
This would typically include Ebola, Zika, Yellow Fever and Dengue.2
2.2 Biological warfare and terrorism
Although many politicians and scientists have pointed at a Wuhan wet market as the source of the coronavirus, other theories understandably serve to contradict. One such alternative relates to biological warfare or bioterrorism. Before discussing the origin of the virus in more detail in chapter 3, I wanted to consider the implications and history of such a theory.
Also known as germ warfare, the concept of biological warfare has been around for at least three millennia, and examples can be traced back to the fourteenth century BC (Barras & Greub, 2014). There is a distinction to be made between biological warfare and bioterrorism. The former would usually constitute a country-on-country attack, while the latter would be performed by a terrorist group that is likely to be working to a different agenda.
One biological weapon that has been used in a number of terrorist attacks is anthrax, although, to date, it has only been used in very small quantities. Even so, concern remains over the potential long-term effects of a large-scale anthrax terrorist attack on a metropolitan area. This is presumed likely to be more devastating than a nuclear attack.
During World War II, the British tested the effectiveness of anthrax on the Scottish island of Gruinard. It was concluded that had, for example, Berlin been bombed with anthrax-based biological weapons, it would still have been uninhabitable at least 30 years later (Cole, 1988). By comparison, the rebuilding of Hiroshima after the dropping of the first atomic bomb in 1945, started within four years (Blackford, 2007). Estimated casualties from a mass bioterrorism attack using agents, such as anthrax, smallpox or plague vary considerably from half a million to 30 million (Clark, 2007) and (Richardson, et al., 2007).
In the 1970s, the United Nations initiated the Biological Weapons Convention (BWC), which came into force in 1975. This BWC was better known as the Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on their Destruction (United Nations, 2017). However, this did not really address any ambiguities, doubts or suspicions that countries may have harboured regarding other countries biological warfare capabilities and their subsequent compliance with the BWC.
“Only 16 countries plus Taiwan have had or are currently suspected of having biological weapons programs: Canada, China, Cuba, France, Germany, Iran, Iraq, Israel, Japan, Libya, North Korea, Russia, South Africa, Syria, the United Kingdom and the United States.
There is widespread consensus against the possession and use of biological weapons. Most countries are party to the Biological and Toxin Weapon Convention, but there is no way to know whether countries are complying with their commitments.”
(NTI, 2015)
Regardless of whether a biological warfare or terrorist attack was launched on a specific target using a biological agent, such as anthrax, apart from perhaps the scale of the attack, the end result would be the same. For the purpose of this chapter, the terms biological warfare, germ warfare and bioterrorism should be considered as interchangeable.
“Bioterrorism is the deliberate release of viruses, bacteria, or other agents used to cause illness or death in people, animals and plants. They (the virus and bacteria, etc.) are typically found in nature.”
(Costgliola & Quaqliata, 2008, p 7)
Biological terrorism is something that has captured the imagination of television and movie producers. In the BBC series ‘Spooks’, Season Six, Episode One, saw MI5 operatives racing to stop a member of a rogue government unleashing a bio-weapon in the UK. Similarly, the third season of the US production of ‘24’, followed the exploits of Jack Bauer and the fictitious Counter Terrorism Unit, while the team attempted to prevent the release of a deadly virus in Los Angeles. Various movies followed the bio-terrorism theme, the first of which I remember seeing was entitled ‘The Satan Bug’, which is just one of several from that genre now listed on IMDb.
Terrorism that attacks a target using weapons of mass destruction (WMD) as its modus operandi, is still in its infancy, with few examples recorded to date of actual incidents. Such an attack would involve chemical, biological, radiological or nuclear (CBRN) based weapons. However, within the UK, the country’s risk register specifies that a small-scale WMD attack, which could include a bioterrorism attack, is considered to have a ‘medium’ probability over the next five years. Moreover, the corresponding relative impact is also recorded as ‘medium’.
2.2.1 Historical use of biological weapons
There is evidence of Russia allegedly targeting defected former KGB officers on UK soil. Using the chemical nerve agent, Novichok, Sergei Skripal was targeted in 2018. In 2006, the lethal radiological agent polonium-210 was used to kill Alexander Litvinenko. Moreover, while working in London, dissident Bulgarian Georgi Markov was also assassinated, allegedly by his country’s security services. A micro engineered pellet containing ricin that was fired into his leg from an umbrella. Of these three state-enacted examples, only the use of ricin was actually a biological attack.
Statistically, the use of WMD by terrorists has averaged eight per annum globally since 1970. To date, if the single terrorist objective was mass casualties, then a combined total of 640 fatalities over that 50 year period (>13 per annum) does not represent a major success. The bomb and bullet still remain much more accessible to terrorists than WMDs, although an increase in the use of knives and vehicle-ramming attacks has certainly been noted.
The UK’s National Counter Terrorism Security Office (NaCTSO) position on the threat of WMD-related terrorist attacks is:
“The likelihood of a Chemical, Biological or Radiological attack remains low, largely due to the difficulty of obtaining the materials and the complexity of using them effectively.”
(Clark, 2012)
However, as an aside, perhaps it is worth noting that NaCTSO makes no such similar claim about nuclear weapons. UK security services endorse the NaCTSO view, and its website says of chemical, biological and radiological devices:
“To date, no such attacks have taken place in the UK. Alternative methods of attack, such as explosive devices, are more reliable, safer and easier for terrorists to acquire or use. Nevertheless, it is possible that Al Qaida, ISIL or other terrorist groups may seek to use chemical, biological or radiological material against the West.”
(MI5, 2020)
To date, chemical weapon attacks appear to have been terrorists’ preferred WMD. Since 1974, there have been close to 400 WMD terrorist attacks chronicled, although, to date, no nuclear attacks have been documented. Fatalities have resulted from the chemical and biological but none from radiological terrorism (US Department of Homeland Security based at the University of Maryland, 2019).
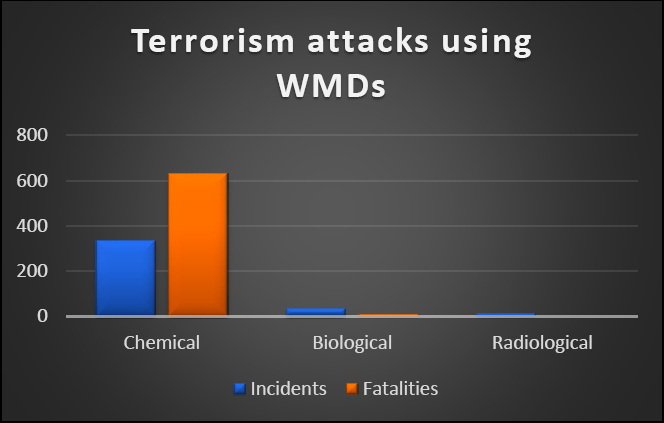
Figure 1: CBRN terrorist attacks from 1974-2018
Anthrax is just one of several lethal biological agents. Its use by terrorists immediately following the 9/11 Twin Towers terrorist attack in eight separate incidents in the US, killing six, accentuated the existence of a bioterrorism threat (Brett, 2003). Anthrax can be found in nature and is common in livestock that can pass it to humans. However, unlike other biological agents, anthrax cannot be passed from human to human. To be effective, the victim must inhale or ingest anthrax spores, or an open wound be contaminated.
The UK National Risk Register (NRR) for 2017, 2015 and 2012, while recognising the threat, only posted a threat rating of ‘medium’ for small-scale CBRN attack and ‘medium-low’ for a large-scale CBRN attack. However, the more recently published 2020 UK NRR has split the CBRN threat into ‘small’, ‘medium’ and ‘large’ CBRN attacks. Furthermore, while the ‘small’ and ‘medium’ attacks have been classified as ‘medium-low’, the large-scale attack has been upgraded to ‘medium’. The 2020 version is available from:
www.gov.uk/government/publications/national-risk-register-2020.
Since 1981, several examples of bioterrorism using anthrax have been recorded in the US. In addition, there have also been cases where ricin, botulinum, salmonella and HIV/AIDS were used. While the majority of incidents occurred in the US, Israel and Japan were also targeted (US Department of Homeland Security based at the University of Maryland, 2019).
An alternative bioterrorism weapon is ricin, which is a naturally occurring toxin extracted from castor beans. In November 2011, the FBI announced the arrest of four US citizens who planned to manufacture ricin and expose other US citizens to the deadly toxin (Federal Bureau of Investigation, 2011).
Palestinian suicide bombers have been known to regularly combine the traditional use of explosives with biological and chemical agents (Cole, 2007). AIDS-contaminated blood, rat poison and hydrogen cyanide have been used to maximise the effect of the terrorist acts. This puts not only any survivors of the blast at greater risk, but also first responders, too. Cole also highlights the psychological effects generated by the biological anthrax attacks in the US in 2001, demonstrating that the fear factor associated with this type of terrorist weapon is substantial.
More recently, concern was expressed in Forbes during 2014, regarding the bioterrorism intentions of the so-called Islamic State using the Ebola virus. Either a lone wolf or groups infected by the Ebola virus would act as carriers of the contagion:
“ISIS may already be thinking of using Ebola as a low-tech weapon of bio-terror, says a national security expert, who notes that the ”Islamic State of Iraq and Syria” and terror groups like it wouldn’t even have to weaponize the virus to attempt to wreak strategic global infection.”
(Dorminey, 2014)
Although ISIS has since lost some of its power base in Syria and Iraq, it would be premature to dismiss its presence as a terrorist threat.
Writing in Scientific American, also in 2014, Dina Fine Maron posed the question: “Weaponized Ebola: Is it really a bioterror threat? What would it take to hijack the virus in West Africa and turn it into a bioterror agent elsewhere?” This train of thought was further supported in 2015 when it was reported that the UK’s top-secret military research unit at Porton Down had been assessing the use of Ebola as a bioweapon.
“The heavily redacted document, which has been released under the Freedom of Information Act, reveals that the unit was asked last October to provide ‘guidance on the feasibility and potential impact of a non-state actor exploiting the Ebola outbreak in West Africa for bioterrorism’.”
(Clark, 2016, p 245)
2.2.2 Classification of biological agents
The Centre for Disease Control (CDC) has created a set of criteria for categorising biological agents. They are grouped into categories A, B or C based on the ease of transmission, severity of morbidity and mortality, plus the likelihood of use.
Agents can be delivered via food or water, and in some cases by airborne transmission. While the majority of the agents listed may result in the death of anyone being exposed, some, such as smallpox, are contagious, while others, such as anthrax, are not.
One has to keep in mind that if a biological attack uses an agent that is a contagion, it may well be difficult to control, and any subsequent infection proliferation could develop into a pandemic. If this attack is state sponsored, one can only assume that the originating state not only has the biological weapon capability, but also a stockpile of vaccines and appropriate medications (e.g. antivirals, antibiotics, etc.) that would be used to protect its own citizens.
The highest threat level in the CDC’s criterion, Category ‘A’, contains the biological agents anthrax, botulinum toxin and ricin, which have already proved to be terrorist weapons of choice. Also included in this category is the Plague (Yersinia pestis), Smallpox (variola major), plus viral haemorrhagic fevers, such as Ebola (CDC, 2018).
1 Ebola, AIDS, Zika and SARS were all unknown infectious diseases before they exploded onto the scene.
2 Some, but not all of which, now have safe, effective vaccines.