12
Near-Miss Incidents
To many laser users, the concept of tracking near misses is so far from their conscientious it might as well not exist. This author has to say, outside of procedural violation records of laser near misses and any corrective actions from them are far and few between. In recent years, the near-miss tracking has become more real, but still just a twinkle in the eye of laser safety officers (LSOs). As a result, the tracking of near misses does have a concrete value.
Why Track Near Misses?
In simple words, they are a warning that should be taken to heart. They usually represent an unsafe condition or practice, that is, uncorrected can lead to a real injury. Few of these are reported, investigated, or have corrective actions taken. Why? Because it was a near miss no one was hit, someone got away lucky, why cause trouble, why admit a mistake? Why report? How are you going to feel when someone else is injured repeating just what you did, for they did not understand a risk or flaw existed?
Following are near-miss reports, covering procedural, technique, engineering, and human element issues.
Case 1: Human Error and Response
Occurrence Report Number: NA—SS-SNL-5000-2006-0004
The incident occurred at Air Force Facility; November 1, 2006, at 5:45 MST involving Air Force and subcontractor personnel, conducting a laser test.
At a staff meeting on November 2, 2006, the Department Manager was briefed on the previous night’s test and told of an equipment anomaly during the trial. Further information was requested from the Air Force operators. On Monday morning, November 6, 2006, the project manager, principle investigator (PI) and the Environment, Safety & Health (ES&H) coordinator reviewed the information and concluded that a laser beam release had occurred when subcontractors were in a nominal hazard zone (NHZ). It was concluded that this constituted a near-miss event and reporting was immediately initiated.
DETAILS
On November 1, 2006, at approximately 5:45 MST, two subcontractors were working in the experimental facility when the beam from the laser (Class 3B) was inadvertently released into the facility. The beam was released by an Air Force safety officer during a safety check, but as a result of not following the correct procedures. The Air Force safety officer was performing a shutter test, without a second beam block in place to prevent the release of the beam. The beam block had been removed during the first safety check, and had not been replaced for the second test. The Air Force safety officer was new (first time working the experiment).
At the time of release, the subcontractors noticed a charge-coupled-device (CCD) camera behaving erratically. The subcontractors asked the Air Force safety officer about a possible release of the laser, to which the response was initially no, but, in fact, the laser had been accidentally released.
The subcontractors were later informed that there had been a temporary release of the beam. The subcontractors were not in the beam path; however, they were in the facility, which is included in the NHZ when the laser is present. The beam was shuttered within seconds of the release. They were not wearing the appropriate eyewear because they were not aware of the existence of the presence of the laser. Therefore, they were unaware of the resultant NHZ. The subcontractors were sent for a medical inspection of any potential exposure damage. They received no exposure damage.
MANAGEMENT SUMMARY
During a laser test, a U.S. Air Force officer failed to follow procedures and inadvertently released a Class 3B laser beam within an experimental facility at the Air Force Base while two subcontract employees were working in the building. The two employees were not in the beam path, but were within the laser’s NHZ. The employees were not wearing laser eye protection, and were sent to the site medical facility for the evaluation of any potential eye-exposure damage. Although results were negative, it was learned that this event was a near miss and reporting was initiated.
Digging deeper here is a more complete incident summary:
Two subcontractors were working in the experimental facility there when the beam from the laser (Class 3B) was inadvertently released into the facility. The beam was released by an Air Force safety officer during a safety check, as a result of not following the correct procedures. The test director was doing a shutter test, without a second beam block in place to prevent the release of the beam. The beam block had been removed during the first safety check, and had not been replaced for the second test. The Air Force safety test director was new (his first time running the experiment) and was not adequately trained for the job by the Air Force staff.
At the time of release, the subcontractors noticed an instrument (CCD camera) behaving erratically, which they quickly surmised was due to the presence of the laser. They immediately informed the safety director of the release, and instructed him to shutter the beam. The contractors were not in the beam path; however, they were in the NHZ and were not wearing the appropriate eyewear. They do not believe they had any exposure damage; however, they are being sent to medical inspection to confirm that fact. Steve Babcock was a spotter on the range at the time, however, he was not in the NHZ, and was therefore not at risk.
The incident was discussed with the Air Force personnel. A test was performed on Thursday night, after assessing the situation, and taking the initial corrective action of replacing the safety test director with a more experienced individual. We did not report the incident to Operational Reporting Procedure System (ORPS) at that point of time, mistakenly supposing that because it was an Air Force facility, and the Air Force was investigating, that we did not need to do so. After further consideration, they were contacted to seek guidance on whether we needed to report further or not.
CORRECTIVE ACTIONS
Air Force safety test director replaced with more experienced Air Force personnel.
Individuals with potential exposure risk sent for medical review to assess any health risks (eye damage).
Incident reports and suggested improvements solicited from involved parties.
An initial suggestion to be implemented, if possible, is the addition of engineering controls in the form of an interlock switch controlled by experimental personnel. This will eliminate inadvertent releases before experimental staff being fully prepared and mitigate potential human communication errors.
As a short-term solution, individuals will only open the laser port into the facility when necessary, and will wear goggles always while that port is open.
Case 2: Search Failure and Too Clever Engineering
Occurrence report number SC—TJSO-JSA-TJNAF-2006-0005
INITIAL DESCRIPTION
About 10:30 am on Friday, December 1, 2006, at a Free Electron Laser Facility, free electron laser (FEL) control room staff noted the presence of a worker in FEL Lab no. 1. Lab no. 1 had received less than 1 minute of FEL light at the time and the lab was immediately saved (laser light delivery stopped). FEL Lab no. 1 had undergone a sweep to remove all workers to initiate exclusionary state (no one was allowed in Lab no. 1) laser operations. The experimental configuration was such that the laser light was delivered in an isolated area, and rope barriers were in place to prevent access to the experiment. The worker did not receive any injury.
IMMEDIATE RESPONSE
Within a minute of laser beam delivery to Lab no. 1, The FEL control room duty officer saw that the Lab no. 1 lights had been turned on and immediately saved Lab no. 1. This action released the Lab no. 1 magnetic door lock. The worker (a Hampton University technician supporting a laser experiment) then left Lab no. 1. There were no injuries to the worker, and there were no ionizing radiation or radioactive/hazardous materials involved with this near-miss event.
The duty officer then terminated all FEL operations and contacted the FEL facility manager. The FEL facility manager concurred that all FEL operations should cease. An electronic record was posted stating that no FEL operations were permitted.
The FEL facility manager immediately contacted the associate director (AD) for the FEL division, lab senior management, Environment, Safety, Health & Quality Division, and the DOE site office. An event investigation team was named and the team began event to follow up at 11:00 am.
The worker was examined at a clinic by the lab physician during the afternoon. The examination verified that the worker had not received any injury as a result of this event.
Digging deeper here is a more complete incident summary:
The event investigation team’s causal analysis determined that the direct cause of the event was an FEL staff member’s failure to do a thorough sweep of the Lab no. 1 as required by the Laser Safety Operating Procedure. A properly conducted sweep requires an entire lab area search to verify no one is present. Contributing causes include the following:
New equipment had been recently added to Lab no. 1 that reduced the sweeper’s field of vision.
The technician was using a computer that was not used in normal operations.
The sweep is time-limited to 1 minute duration (by the safety system software), which contributes to some urgency in getting the sweep done quickly.
Since Lab no. 1 had been in an open state, and this worker was not involved with the lasing aspects of the experiment, no laser-specific training was required. This lab-specific training instructs workers that the crash button on the laser personnel safety system (LPSS) must be pushed as the exit button is inoperable in the exclusionary mode (this is the status immediately after the sweep and before/during laser delivery).
The exit buttons are not well engineered from a human engineering standpoint. There is no indication that they do not function when the lab is in exclusionary mode.
Two phases of corrective actions are as follows.
INTERIM ACTIONS
Immediate FEL operations stand down.
Briefing of all lab operational staff at the lab’s two daily operations planning meetings. The outside FEL physics user group also receives a briefing on the event.
The FEL lab sweep procedure will be modified until permanent LPSS changes are in place. These interim changes include the use of two people for all presweeps with no time limit. Once the presweep is done, one person performs the sweep procedure called for in the procedure. During the sweep, the sweeper will push the mounted simulated sweep buttons that direct the sweep to all relevant parts of the lab.
Personnel will be trained in the new sweep procedure.
Review this event with the users involved. The Jefferson Lab director communicated the importance of safety, and the lab’s safety expectations to the PIs leading this experiment.
A sign will be posted near the exit buttons in all FEL labs indicating which button to use if the exit button does not work.
The lab LSO will brief all non-FEL system safety supervisors of this event by December 11. This briefing will also determine if there is any extent of condition applications in other non-FEL activities.
Note: All interim actions were completed by December 4 except for action 7.
PERMANENT ACTIONS
Two to four sweep buttons will be placed in each FEL lab to verify that the sweep goes to all portions of the lab. There will be a sweep button in each walk-in hutch as well.
There will be a verbal announcement that a sweep is occurring as the sweep begins.
There will be a verbal announcement that lasing is to begin after the sweep has taken place and 30 seconds before the beam is provided to the lab.
Ensure that FEL users are familiar with this event and applicable FEL protocols prior to initiating experiments.
More Background Details for the Curious
The FEL is a high-power laser operating at wavelengths between 0.9 and 10 micrometers. It is tunable over each set of mirrors being used. The light is produced in a radiation-shielded vault and transported through an evacuated transport system to one of seven user labs in the FEL facility. Each lab can be swept (cleared of all personnel), locked up, and brought up in a state of Laser Permit. If an interlock is tripped or a crash button is pushed, the lab is crashed and transitions to an open state. If an open state is required, the FEL operator can safe the lab using the laser control system. When the lab is in an open state, access is permitted to anyone and the only training required is the training required to be on the accelerator site. When one wants to put the lab into a Laser Permit state, an approved laser user or FEL operator sweeps the lab according to a sweep procedure documented in the Laser Standard Operating Procedure. There are three possible states in a lab when a lab is in laser permit. In Exclusionary mode, no one is permitted in the user lab. This is the default state for a lab. In Hutch mode, the laser is confined to interlocked hutches inside the lab. In alignment mode, the power to the lab is restricted to low levels so that a user with laser-safety eyewear can align the laser beam to their apparatus. Trained personnel (identified by a radio frequency identification [RFID] badge) can enter the lab when it is in alignment mode (if they are wearing appropriate laser-safety eyewear) or in hutch mode. No access is permitted in exclusionary mode. Egress from the lab is accomplished by pushing an exit button on the door or the LPSS. These buttons only function in alignment mode or hutch mode. To gain egress in exclusionary mode, it is necessary to use the crash button on the LPSS chassis. This is taught to all approved laser users.
A sweep consists of presenting one’s RFID card, entering the lab, verifying that all personnel have exited the lab, pushing an initiate sequence button, exiting the lab, and presenting one RFID card a second time. In this case, the lights were turned off after pushing the initiate sequence button. Thirty seconds after pushing the initiate sequence button, the lab goes into a state of laser permit. During this time a warning beacon is illuminated and a warning alarm is sounded. When the lab is in laser permit, the warning alarm is turned off and the warning beacons stay on.
First, the lab was locked up and saved several times during initial checkout of the experiment’s diagnostics.
Subsequently, it was determined that a camera had to be replaced so the lab was saved and three technicians and one of the FEL operators entered the lab to change it out. During the entry, a user associated with the LPSS experiment went into the lab to use a computer along the north wall to check his e-mail. Once the camera was replaced, the three technicians left the room and the FEL operator swept the lab to bring it into laser permit. This was at about 10:28 am. The start of the sweep was announced by the operator, but the user did not hear him. The FEL operator did not do a thorough sweep and did not see the technician. Following the sweep, he pushed the initiate sequence button, turned off the lights, and exited the lab.
The user realized that the lab was going into laser permit and tried to leave the lab using the exit button on the door to leave.
When the lab is in exclusionary mode, the exit buttons are nonfunctional. Instead, it is necessary to hit the crash button to leave the lab in exclusionary mode, so pushing the exit button did not release the mag locks on the door, and the user was unable to exit. To notify the control room that he was in the room, he turned the overhead lights on and off and then left them on, with the intention of bleaching the camera response to alert the control room staff that there was a problem. He also ensured that he remained at the door facing with his back to any potential stray laser beams. The user had the required Laser Safety Orientation (SAF 114O) and Laser Medical Approval (SAF 114E) to be a user. He did not have, nor was he required to have laser-specific training to be in the lab when in the open state.
The FEL operators sent 25 W of FEL light at 990 nm into the lab. The light was directed through the optical transport onto a power meter for a total of 1 minute (see Figure 12.1). When the FEL operator saw that the lights had been turned on in the lab, he immediately saved the lab. This was at 10:30 am. When the lab was crashed, the technician was able to immediately exit the lab.
The duty officer then terminated FEL operations and contacted the facility manager. He concurred that all lasing operations should cease and posted an electronic record called an FLOG indicating that FEL operations were not permitted. He then contacted the AD, the lab LSO, and the laser system supervisor (Figure 12.1).
Management Summary
Figure 12.1
View of Lab 1 from entrance door. Computer workstation is located along the wall on the right side of the lab, behind the magnet setup.

During laser operations in the FEL Lab no. 1, control room staff unexpectedly discovered the presence of a worker in the laboratory after a sweep to remove all workers was performed and laser operations were underway. The laser light was in operation for less than 1 minute when the worker was discovered and the laser light was immediately stopped. There were no injuries to the worker. An investigation was initiated.
Lessons Learned, Including ES&H Manual changes (if any):
A persistent problem with administrative controls in safety systems is that their effectiveness depends on the diligence of the person enforcing the control. The importance of this diligence must be continually reinforced over time so that incidents like this do not occur. Engineering controls can force a sweeper to take their time and cover the required territory, but are no substitute for being careful in the sweep. It is also important to continually stress that personnel take whatever time is required to do a careful sweep and not rush the sweep.
Another lesson learned is to consider human engineering when designing the user interface for a safety system. Inexperienced users are reticent to push crash buttons as they think they will break something. They would rather push an exit button. If an exit button is present but non-functional, they will typically be confused and not know what to do. The best solution is for the exit button to be the crash button.
Finally, it is important to consider how things work when things do go wrong. Even if an event is unlikely, it is important that things work as they should during the event.
Case 3: Legacy and Funding Event
During the installation of a new laser interlock system at the ATF, some potential safety risks were discovered in the previously existing system. The interlocks are very complex as there are two Class 4 lasers whose outputs are sent to different places to excite the photocathode that provides electrons for the Linac. They are used in different rooms as part of the various experiments and there are many different configurations on the beam lines. The complexity is reflected in the test procedures where there are 246 steps, many with multiple-step check-offs.
The project had been transferred between groups with varying funding resources. It was determined that both the radiation and laser interlocks were beyond the expertise of the new group and required outside expertise. A memo-riam of understanding was developed.
C-A Department has the responsibility to maintain or modify the ATF access control system hardware and maintenance procedures. This includes, but it is not limited to logic diagrams, wiring diagrams, test procedures, interlocks, interlocked gates, beam crash buttons or cords, reset stations, critical devices and Radiation Safety Committee review of same.
To facilitate this, a complete set of drawings for both systems were requested and received. A management review led to the following memo:
Safety Systems
Laser Interlocks: The ATF has a complex set of interlocks that has been weakly supported by the institution interlock group leaving the ATF with a system that is not properly documented for the system that is in place. Changes over the years are not documented and the procedures for testing do not properly cover the current configuration. Furthermore, those who designed and implemented the system are refusing to support the ATF even as purchased services. This is a critical situation. We are actively trying to get the C-A Department to review and take responsibility for the maintenance and testing of the ATF interlocks, but the cost of redoing the system may be prohibitive.
Testing and recertifying the laser interlock system by adding to the test procedures the items known not to have been included, believing the rest of the test procedures to be complete. At the time we did believe that we could not verify the completeness of the test procedures because we were concerned we never had complete drawings. At the time of the turnover from one group to another department, the previous engineer stated that all the changes to the drawings had been completed but changes to the test procedures had not. The changes to the test procedures were completed in July 2004. The system continued to operate believing that all was in order. However, this could not be independently verified. To this end it was decided that the system would have to be replaced, completely re-documented, verified, and certified. Money was allocated for this and with the help of C-AD has now been done as of June 6, 2007.
Interlock Tests
ATF procedures, in compliance with the SBMS subject area, require laser interlocks to be tested every 6 months. Original checklists are kept in the ATF control room with copies sent to the department’s Safety and Training Office where the manager of Environment, Health, Safety, and Training program reviews them.
The test procedures were originally developed by the institution and since (working with the C-AD) have been modified to remove testing for devices no longer physically present, add testing for a device added into the interlock chain, and redefine some areas (two separate areas merged into a single area). At that time, the department chair requested assistance from the institution chair who permitted their interlock engineer (person involved in the original design, implementation, and testing) to help facilitate the changes. When the modified procedures were acceptable to both the groups and C-A Departments, they were adopted and published.
Concerns That Arose
In replacing the old laser interlock system with the new one, the plan was to replace the Programmable Logic Controller (PLC) with the same type currently used by the C-AD interlock group for their interlocks to use the same programming language and take advantage of their expertise with this hardware and software. In principle, the new controller boxes had the same inputs and outputs as the old ones, so replacing the new boxes compatible with the new PLC and language should have been easily done and no new wiring was expected. The old bundle of wires simply had to be plugged into the new boxes. After this was done, the system began to be checked and discrepancies were found.
It was found that the drawings as given from the institution were not complete or accurate. ATF personnel found approximately 30 errors in the existing drawings.
In addition, it is doubtful that a fully functional test had been done on the status indicator boxes as there was a light-emitting diode (LED) that was wired backward and could have never worked.
In certain cases, an indicator light, that implied two shutters were closed, was lit when only one shutter was actually closed. Other laser status panel on LEDs could not be correctly controlled because they were hard-wired to a shutter open switch. In order for the LEDs to be correctly controlled, they need to be independently driven by the interlock system.
The yttrium aluminum garnet (YAG) shutter status of the LEDs on the CO2 room enclosure did not reflect the position of the YAG shutter because the LEDs were not correctly wired. The shutter open LED would light whenever the CO2 to high-bay pass-through button (means to enter the inter-locked area by authorized personnel) was pressed. The shutter closed LED would light when the 10-micrometer imminent LED was on. While these wiring problems did not add additional risk to personnel, they are indicative of the lack of a full functional test.
Finally, it was apparent that the normal best practices for color coding different sets of wires were not done as most of the wiring was the same green color.
Safety Implications
The improper lighting of status indicators was viewed by users to determine which laser eyewear to use put them at potential risk for eye damage. This authorized user list was limited in number to those specifically included in the approved Experimental Safety Reviews. These people had the proper training, including the initial eye examinations given to authorized laser users. They are not permitted to do laser alignments or maintenance. Their use of laser light was limited to their experimental equipment.
The incorrect indicators of laser safety shutters state put users and staff at additional risk.
Before the transfer of the ATF to the department, the institution was responsible for the design, documentation and installation, and programming and testing of the laser interlock and radiation systems. Ilan Ben-Zvi, who used to head the ATF, remembers the institution’s running functionality tests of the whole system as some points in the past, but it would appear that rewiring must have been done at some point as the backward wiring would have been found at that time as well as the false indication that two shutters were closed when, in fact, the indicator light was lit when only one was closed.
I did not know that the full interlock test procedures did not cover each and every item in the system and that it took five to six days. I was informed this morning that he didn’t know this himself until last week. I presumed that when there was a modification, the interlock test procedures tested the whole system.
Analysis to This Point
Unlike the interlocks for radiation, I do not believe the areas covered by laser interlocks alone are subject to the Accelerator Safety Order, as Ron Gill (Physics Department’s ES&H coordinator) and I discussed this morning.
Unlike the area encompassed by the interlocks for radiation (which is an exclusion zone when radiation is present in the Experimental Hall), the laser areas are configured for occupation by properly trained persons (with the proper personnel protective equipment (PPE)) when the interlocks are on and laser light is present in the rooms. This allows properly trained people to make adjustments, align the lasers, maintenance, and approved experimentation.
The status indicator lights are not required but are part of the inter-lock safety system as they get their information from the interlock circuitry, and users will usually use this information to choose the correct eyewear.
Laser safety eyewear is intended as an additional control to reduce risk of eye damage and is required by the ANSI (American National Standards Institute) standard. The laser SOP is used to analyze the hazard and specify the optical density. All of that is in order.
There is no reason to believe that any user received any eye damage although the potential was there.
I believe it is prudent to see if the SDL has a similar situation. Have they had a fully functional test? Do they rely on indicator lights for eyewear? If so, is that system working properly?
Looking at the categorizer’s procedure, it might come under the following but is at the discretion of line management and not required to be reported: Group 10—Management concerns/issues
(2) 1–4† An event, condition, or series of events that does not meet any of the other reporting criteria but is determined by the facility manager or line management to be of safety significance or of concern to other facilities or activities in the Department of Energy (DOE) complex. One of the four significance categories should be assigned to the occurrence, based on an evaluation of the potential risks and the corrective actions taken.
(3) 1–4† A near miss, where no barrier or only one barrier prevented an event from having a reportable consequence. One of the four significance categories should be assigned to the near miss, based on an evaluation of the potential risks and the corrective actions taken.
Present Status
There is a new interlock system in place. This system is fully documented with a new set of drawings, the hardware has been installed by ATF personnel, the controlling software was written by the C-AD interlock group, tested by C-AD interlock technicians and was reviewed and certified by C-AD personnel. The status indicator lights are currently not part of the system but will be added to it, documented, and test procedures will include their testing. Until then, no users will be permitted to be in the laser interlocked areas until the status lights are operational and certified to be working properly.
In the future, any modifications will require a full functional test as well as properly documented updates to drawings.
Case 4: Deliberate Bypassing of a Safety System
During a visit in October 1998, we performed a series of integrated dry runs and discovered that three interlocks on the experiment room door were taped in a bypassed condition. The preliminary inquiry concluded that the bypassing might have taken place the preceding evening, when site personnel were ensuring that two Class 4 lasers were correctly aligned for the integrated dry runs. The test group director has prohibited the operations of x-ray and laser equipment until the incident was fully evaluated. If such equipment is operating while an interlock is overridden, entry into the area will not shut the equipment down, and personal injury could occur.
A follow-up investigation determined that facility workers attempting to identify which interlock was connected to the laser systems had systematically taped the door interlock devices in a bypassed condition, in violation of the approved operating procedure. It was also determined that the facility staff forgot to remove the tape before the dry runs. The review concluded that since the experiment room door had cipher locks and access was administratively controlled, there was no chance of personnel exposure of injury.
Case 5: Wanting to Be Helpful but Just Following Through Not Thinking
September 2006
A plumber asks a researcher (visiting scientists) to let him into an interlocked laser lab. The researcher puts in the access code, allows the plumber to enter, and he returns to his office. Oh yes, the lasers were running in the laser lab. The PI of the lab is in the lab doing a laser alignment. He sees the plumber (without eyewear) and escorts him out.
Case 6: Near Miss at Los Alamos National Lab
September 2000
A service man is working on an LSR flow cytometer (9/20). These units contain from 2–3 Class 3B lasers. He removes the top enclosures and housing over the lasers. The service man leaves the unit in this way and plans to return in a few days to complete the repair. Three days later, a group leader observes two employees standing over the unit, looking inside of it with the laser on.
Case 7: Near-Miss Fiber Optic Example 1
Two workers were moving fiber cables when they inadvertently viewed a green light emitting from one of the fiber cable ends.
Two laser operations were being performed simultaneously:
Workers were in one room attempting to connect the fiber optics to the patch panel.
Laser personnel were in another room aligning their interferometer using the attenuated laser beam.
Following discovery of the laser light, the laser system was de-energized. The output from evaluation concluded that the workers did not sustain any eye injury.
Case 8: Near-Miss Fiber Optic Example 2
The laser operator had inadvertently left the fiber optic connected to the laser beam.
The only control to keep the laser light out of this pathway was administrative (a checklist), which relied on the laser operator to disconnect or block the laser light from the input fiber. However, the checklist had no step to ensure that the operator disconnected or blocked the laser light.
There was no labeling of the fiber optic cables, patch panel connections, or junction boxes as required.
The laser enclosure lid had no safety interlocks as required.
Neither the workers nor the laser operators had a laser system key control during their work activities. The workers were unaware of laser operations in the laser room (no communication).
Case 9: Near-Miss-Labeled Case 2 Really Class 3B
A labeled Class 2 laser, used in a high-resolution ruby fluorescence high-pressure measurement system, had its beam power level measured and found to be in the Class 3B power output range. The laser was supposed to have a nominal output no greater than 1 mW, but the measured output was 18 mW.
Optiprexx 532 nm laser systems procured before 2007 may be at a higher class power level than advertised.
Near-Miss Reporting
A thorough near-miss investigation has the potential to identify overlooked physical, environmental, or process hazards; the need for new or more engineering controls or safety training; or unsafe work practices. The supervisor of the employee involved in the near miss is responsible for conducting the investigation and, when appropriate, ensuring that corrective actions are taken. The depth and complexity of the investigation will vary with the circumstances and seriousness of the incident. Investigators must maintain objectivity throughout the investigation. The purpose of the investigation is to uncover any factors that may have led to the accident, not to assign blame.
The first is all narrative.
Background information: Site location, department, supervisor, date, time, year of work.
Witnesses: Self-explanatory.
Description of accident: Most near misses result from an accumulation of events. An accurate, factual description of the accident and the events leading to it can be very helpful. This chronological sequence can be studied to determine how each event may have contributed to the near miss. Include photos or drawings of the accident site, if these will be useful to the investigation.
Factors: Factors, if any, are the conditions in the workplace or actions that contributed to the near miss of this near miss. Examples might include unguarded machinery, broken tools, and slippery floors, not following established procedures, or insufficient training or maintenance.
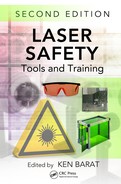
Corrective actions: List actions or steps that could be taken to control or eliminate the likelihood of a recurrence; include not only those that can be accomplished right away (e.g., providing personal protective equipment, installing a machine guard) but also actions such as changes in policy or providing additional training (Figure 12.2).
Figure 12.2
Near-miss report form sample.
Conclusion
The near-miss incident can easily show problems with one’s safety culture or that of others. Therefore, the reporting of near-miss incidents should be supported and employees encouraged to do so. In reality, a hard goal to accomplish, but has a positive payoff.