Personality factors will be addressed that may be associated with substance abuse. Alcohol will be covered as it pertains to the workplace and the symptoms that accompany persistent drinking. Various types of drugs such as marijuana, cocaine, hallucinogens etc. will be discussed.
Before beginning any discussion about substance abuse, some basic vocabulary needs to be defined.
In broad terms, drug dependence is defined as the need or perceived need of a person to continue taking a drug. Abuse is defined only in terms of society’s disapproval. It involves different types of behavior and may involve psychological and/or physical dependence. Addiction is the state of being that includes drug dependence, considered to be compulsive and overwhelming, usually both physical and psychological. Addiction implies the risk of harm and need to stop use by withdrawal or abstinence, whether the addict agrees or not. Tolerance is a need to increase the dose progressively in order to produce the effect originally achieved by smaller amounts. A withdrawal syndrome is characterized by physiological changes that occur when a drug is discontinued, such as convulsions, violent shaking, twisting, sweating, vomiting, delirium, etc.
A single definition for drug dependence is impossible. The term drug dependence of a specific type emphasizes that different drugs have different effects.
Drug abuse can include the following:
1. Experimental and recreational use of drugs
2. Use of drugs to relieve problems or symptoms
3. Use of drugs to relieve problems or symptoms, which leads to a dependency
Recreational drug use has increasingly become a part of our culture, even though it is not sanctioned by our society. Recreational users tend toward sporadic drug use involving relatively small doses, and they apparently do not suffer harm from their exposure. Recreational use is seldom practiced alone. Most drugs used in this manner are used to obtain a “high” rather than to relieve distress. For this reason, depressant drugs are seldom used by the recreational user.
Two general aspects are common to most types of drug dependence:
1. Psychological dependence involves feelings of satisfaction and a desire to repeat the use of the drug in order to produce pleasure or avoid pain. The mental state is a powerful factor involved in chronic use of certain drugs.
2. Physical dependence is a state of addiction to a drug, accompanied by development of tolerance.
Drugs that produce dependence act on the central nervous system and produce one or more of the following effects:
• Reduced anxiety or tension
• Elation, euphoria, or other pleasurable mood changes
• Feelings of increased mental and physical ability
• Altered sensory perception
• Changes in behavior
These drugs can be divided into two categories: those that cause psychological dependence and those that cause both a physical and psychological dependence. Drugs that cause primarily a mental dependence include the following:
• Cocaine
• Marijuana
• Amphetamines
• Bromides
• Hallucinogens, such as lysergic acid diethylamide (LSD), methylene dioxyamphetamine (MDA), and mescaline
In the United States, the Comprehensive Drug Abuse Prevention and Control Act of 1970 and subsequent changes require the drug industry to maintain physical security and strict recordkeeping over certain types of drugs. The Act also divided controlled substances into five schedules or classes on the basis for their potential for abuse, accepted medical use, and accepted safety under medical supervision. Substances included in Schedule I are those with a high potential for abuse, no accepted medical use, and a lack of accepted safety. Those in Schedules II through V decrease in potential for abuse. Prescriptions for drugs in all these schedules must bear the physician’s U.S. Food and Drug Administration (FDA) license number.
The development of drug dependence is complex and unclear. At least three components require consideration: the addictive drugs, predisposing conditions, and the personality of the user. The psychology of the individual and drug availability determine the choice of the addicting drug and the pattern and frequency of use. Drug dependence is in part related to cultural patterns and to socioeconomic factors. Factors that lead to increased use can include peer or group pressure, emotional distress, sadness, low self-esteem, and stress. The specific effects of each drug may temporarily ease these factors.
Pharmacological factors
With some drugs, after only 2–3days of continued use, some physical dependency may exist for some people. These persons generally have mild withdrawal symptoms, which may have the same symptoms as influenza (flu), but they do not become addicted. Even persons with chronic pain problems requiring long-term administration usually are not addicts. These persons may experience some problems with tolerance and physical dependency but do not develop an addiction. Some substances (i.e., heroin) have a high potential for physical dependence and are more prone to abuse, even when used in a social or recreational setting. Pharmacological effects are important but are not the only factors in the development of drug dependency.
Genetic factors
It is now believed that genetic factors may indeed play a part in the addiction process. These genetic factors may cause a predisposition that, when combined with one or more of the other previously discussed stressors, can more likely produce an addict. This is not to say that everyone with this predisposition will become an addict. It is just another piece of the addiction puzzle.
Personality factors
The “addictive personality” has been a term used by behavioral scientists, but there is little scientific evidence that characteristic personality factors exist. Some believe that addicts are escapists—people who cannot deal with life and choose to run away. Others have described addicts as schizoid persons who are fearful, withdrawn, and depressed. Addicts have also been described as basically dependent and grasping in their relations with others.
Dependence on alcohol
Alcoholism is a chronic illness showing recognizable symptoms and signs in direct relationship to its severity. Experts estimate that alcohol abuse costs the United States more than $223.5billion/year. Dr Tom Frieden, Director of the Centers for Disease Control and Prevention, was quoted as saying in August 2013, “It costs our society billions of dollars through reduced work productivity, increased criminal justice expenses and higher healthcare costs.” (source: www.atlanta:cbslocal.com/.../cdcalcoholabuse.)
An alcoholic is identified by severe dependence or addiction and a pattern of behavior associated with drinking.
1. Frequent intoxication interferes with the ability to socialize and work.
2. Frequent intoxication may lead to marriage failure and work absenteeism.
3. Alcoholics may suffer physical injury and/or be apprehended for driving under the influence.
4. Alcoholics may be hospitalized for delirium tremens (also known as the DTs—the body’s and brain’s reaction to alcohol withdrawal after prolonged use) or cirrhosis of the liver (breakdown of liver function).
The incidence of alcoholism among women, children, adolescents, and college students is increasing. Males outnumber female alcoholics by a ratio of 2.5 to 1. It is generally assumed that 67% of American adults drink alcoholic beverages and one in six will experience some problem with alcoholism.
Families of alcoholics tend to have a higher incidence of alcoholism. Genetic or biochemical defects leading to alcoholism are suspected but have not been clearly demonstrated, although a higher incidence of alcoholism has been consistently reported in biological children of alcoholics as compared to adoptive children. Social factors affect patterns of drinking and consequent behavior. Alcoholics frequently have histories of broken homes and disturbed relationships with parents.
Physiology and pathology
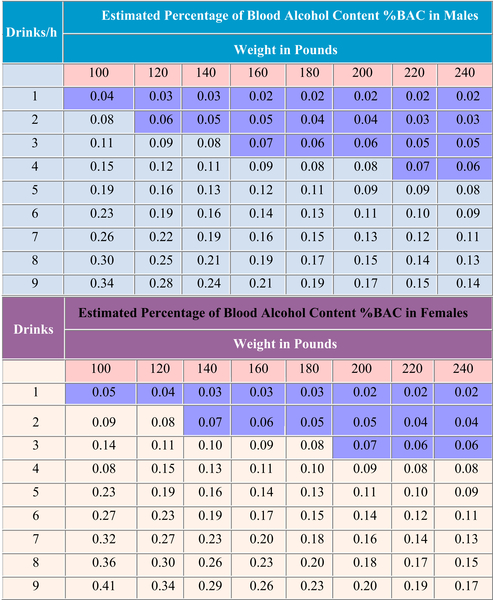
Alcohol is absorbed into the blood, principally transmitted through the small intestine. It accumulates in the blood because absorption is more rapid than oxidation and elimination from the body. Depression of the central nervous system is a principle effect of alcohol. Please see the Alcohol Blood Content chart at the end of this chapter.
The most common forms of specific organ damage seen in alcoholics are cirrhosis of the liver, brain damage, and cardiomyopathy (heart disease). Gastritis is common and pancreatitis may also develop. Irreversible impairment of liver function occurs in some alcoholics. Both the direct action of alcohol and the accompanying nutritional deficiencies are considered responsible for the frequent nerve problems and brain damage. Alcoholic cardiomyopathy (heart disease) may develop after approximately 10years of heavy alcohol abuse and is attributed to a direct toxic effect of alcohol on the heart muscle.
Persons who drink large amounts of alcohol repeatedly become somewhat tolerant to its effects. The physical dependence accompanying tolerance is great, and withdrawal produces a series of adverse effects that may lead to death. Symptoms and signs of alcohol withdrawal usually begin 12–48h after the intake of alcohol has stopped. The main withdrawal symptoms include tremors, weakness, and sweating.
Symptoms and signs
Signs of alcohol use may include slurred speech, dizziness, drowsiness and falling asleep at work, hangovers (including headaches, shaking, nausea, and vomiting), lack of coordination, and lack of inhibition or self-control.
Dependence of the opioid type
Opioid type drugs are considered narcotic and are the most effective pain reliever, used by physicians for surgery, fractures, burns, etc. Opium itself is a dark brown, plastic-like substance that is smoked through a long stemmed pipe. Opium is the dried milk of the unripe opium poppy. The first major attempt to control opium use came in 1909, with a federal act that limited the use of opium and derivatives except for medical purposes. For the most part, opium has been replaced by its more powerful derivatives: morphine and heroin.
Morphine is the preferred drug for relief of pain and is derived from crude opium. Morphine is an odorless, light brown, or white crystalline substance in tablets, capsules, or powder form. It is either injected or taken orally. It acts on the central nervous system as a pain killer (analgesic).
Heroin is processed from morphine, a naturally occurring opiate extracted from the seedpod of certain varieties of poppy plants. It is 2–10 times as potent as morphine. It is extremely popular because of the high it produces. The opium poppy has been cultivated for more than 5000years for a variety of medicinal uses. Heroin was first synthesized from morphine in 1874. From 1898 through to 1910, Bayer, the German pharmaceutical company, marketed it under the trademark name Heroin as a cough suppressant and as a nonaddictive morphine substitute (until it was discovered that it rapidly metabolizes into morphine). One year after beginning sales, Bayer exported heroin to 23 countries.
Heroin is manufactured from opium poppies cultivated in four primary source areas: South America, Southeast and Southwest Asia, and Mexico. Although Afghanistan produces the majority of the world’s heroin, South American heroin has become the most prevalent type available in the United States, particularly in the Northeast, South, and Midwest. A less pure form of heroin from Mexico, known as “black tar”, is more commonly found in the western and southwestern United States. This heroin may be sticky like roofing tar or hard like coal, with its color varying from dark brown to black.
Street heroin is rarely pure and may range from a white to dark brown powder of varying consistency. Such differences typically reflect the impurities remaining from the manufacturing process and/or the presence of additional substances. These “cuts” are often sugar, starch, powdered milk, and occasionally other drugs, which are added to provide filler.
Heroin can be sniffed, smoked, or injected. Mexican black tar heroin, however, is usually injected (once dissolved) or smoked because of its consistency. Like other opiates, heroin is a sedative drug that slows body functioning. People who use it describe a feeling of warmth, relaxation, and detachment, with a lessening sense of anxiety. Due to its analgesic qualities, physical and emotional aches and pains are diminished. These effects appear quickly and can last for several hours, depending on the amount of heroin taken and the route of administration. Initial use can result in nausea and vomiting, but these reactions fade with regular use.
People who use heroin regularly are likely to develop a physical dependence. Withdrawal symptoms (“cold turkey”) may begin within 6–24h of discontinuation of the drug; however, this timeframe can fluctuate with the degree of tolerance as well as the amount of the last consumed dose. Symptoms may include sweating, anxiety, depression, chills, severe muscle aches, nausea, diarrhea, cramps, and fever.
Injection poses the greatest risk of lethal overdose by enabling large amounts of heroin (and additional contaminants, if any) into the bloodstream at once. Smoking and snorting heroin can also result in overdose, especially if a nontolerant user ingests a large amount of potent heroin and/or combines it with other depressant drugs, such as alcohol. Symptoms of a heroin overdose include slow and shallow breathing, convulsions, coma, and possibly death. To avoid fatal overdose, it is strongly recommended that people who use heroin (and their peers and loved ones) be trained to administer naloxone, an overdose reversal drug that has been approved by the FDA since 1971.
The use of dirty or shared needles when injecting heroin can spread deadly infectious diseases, such as human immunodeficiency virus (HIV) and hepatitis B and C viruses. Injecting drugs and/or sharing needles can contribute to other diseases and conditions that may be serious or even life threatening, including endocarditis, embolism or blood clots, botulism, tetanus, and flesh-eating bacteria. Finally, injecting may cause abscesses (a painful skin inflammation) that, in turn, may result in blood poisoning.
Codeine is a weak derivative of opium and is most commonly used in cough medicine and milder pain medicine. It is less addictive than morphine or heroin.
Methadone is a synthetic opiate developed during World War II in Germany. It is considered to be more addictive than heroin and is used to block the withdrawal symptoms of heroin. Methadone may be taken orally or injected. Methadone acts as an opiate agonist that has a series of actions similar to those of heroin and other medications derived from the opium poppy. Methadone is used to reduce and even eliminate heroin use by stabilizing people struggling with addiction for as long as is necessary to help them avoid returning to previous patterns of drug use. It prevents the physical cravings for the drug. Methadone maintenance treatment has been documented in hundreds of scientific studies to reduce crime, death, disease, and drug use. Compared to the other major drug treatment modalities—drug-free outpatient treatment, therapeutic communities, and chemical dependency treatment—methadone is the most rigorously studied and has yielded the best results. There are more than 115,000 methadone maintenance patients in the United States, including 40,000 in New York state and 20,000 in California. It is also now being used in the treatment of severe, prolonged pain in cancer patients.
A strong mental dependency can occur, which creates an overpowering compulsion to continue taking the drug. Tolerance develops, so the dosage must be continually increased in order to obtain the initial effect. Physical dependency will occur with increased dosage and continued use.
Tolerance to and physical dependence on the opioids and synthetic narcotics develop rapidly. Therapeutic doses taken regularly over a 2–3day period can lead to some tolerance and dependence and the user may show symptoms of withdrawal when the drug is discontinued. Opioid drugs induce cross-tolerance. Abusers may substitute one drug for another.
Symptoms and signs
Acute intoxication with opioids is characterized by euphoria (a feeling or sense of happiness and well-being), reddening and itching of the skin, drowsiness, decreased respiratory rate, hypertension, and decreased body temperature. During withdrawal, symptoms begin to appear as early as 4–6h after cessation and reach a peak within 36–72h for heroin. The initial anxiety and craving for the drug are followed by other symptoms increasing in severity and intensity. A reliable early sign of withdrawal is an increased respiratory rate usually accompanied by yawning and perspiration.
Dependence of the barbiturate type
Barbiturates are depressants and are used to induce sleep or to act as mild sedatives or tranquilizers. Mental dependence may lead to periodic or continuous use of the drug which, in turn, can result in a physical dependence after a user ingests amounts considerably above the therapeutic or socially acceptable levels.
Symptoms and signs
In general, those dependent on sedatives and hypnotics prefer rapid-onset drugs, such as secobarbital and phenobarbital. In susceptible persons, psychological dependence on the drug may develop rapidly and after only a few weeks. Attempts to discontinue use may result in insomnia, restlessness, disturbing dreams, and feelings of tension early in the morning. The extent of the physical dependence is related to the barbiturate dosage and length of time that it has been taken.
Barbiturate users may appear as if they are drunk. Their anxiety level will drop, as well as their blood pressure and respiration rate. An abrupt withdrawal from large doses of barbiturates or tranquilizers produces a severe, frightening, and potentially life-threatening illness similar to delirium tremens. Withdrawal from barbiturates carries a significant mortality rate and should always be conducted under medical supervision.
Dependence on marijuana
Chronic or periodic use of marijuana (cannabis) or cannabis substances produces some mental dependence due to its desired effects, but no physical dependence occurs. Marijuana can be used on a periodic basis without evidence of social or psychic (mental) problems. For many users, the term dependence is probably a misconception.
Marijuana use is widespread in the United States and is commonly used in the form of a cigarette. Recently, synthetic tetrahydrocannabinol (THC), which is an active ingredient of marijuana, has become available for research and chemical use. Some controversy exists whether THC is available on the street for drug dealers and users. As of 2014, the sale and possession of marijuana is legal for both medical and nonmedical use in two states, Colorado and Washington. Nineteen other states have laws legalizing marijuana in some form.
Symptoms and signs
Marijuana produces a dreamy state of consciousness in which ideas seem disconnected, uncontrollable, and free-flowing. Time, color, and perceptions are distorted. In general, there is a feeling of well-being, exaltation, and excitement that has been termed a “high”. Many of the psychological effects seem to be related to the setting in which the drug is taken.
Metabolic products of marijuana are retained in the tissues for a long time. For this reason, many persons who undergo a drug screen urinalysis may show byproducts of marijuana in their urine for 30days after use. Lowered testosterone (sperm count) levels have been reported in some males.
Dependence on cocaine
Psychic or mental dependence sometimes leads to an extreme psychological addiction when cocaine is used in high doses. In studies of cocaine use, physical dependence or a tolerance to the drug has never been proven. However, there is usually a strong desire to continue to take the drug.
Cocaine use and the development of addictive behavior have continued to increase in the United States. The smoking of “freebase” cocaine (crack) has become popular. This requires the conversion of the hydrochloride salt to the more combustible form. A flame is held to the material and the smoke inhaled. The speed of onset is quicker and the intensity of the high is magnified. Because this process uses flammable liquids, there have been serious explosions and burns.
When snorted, procaine produces sensations not unlike cocaine and may even produce a high. Powered procaine is widely used to cut cocaine and is occasionally mixed with mannitol or lactose and sold as cocaine. It is sometimes called “synthetic cocaine”.
Treatment of acute cocaine intoxication is generally unnecessary because of the extremely short action of the drug. If an overdose requires intervention, Schedule IV barbiturates may be used. However, the difficulty in breathing that accompanies cocaine intoxication can be worsened with the use of sedatives. Discontinuing the use of cocaine requires considerable assistance and the depression that may occur requires close supervision and treatment.
Symptoms and signs
When cocaine is either injected or inhaled, it produces a condition of euphoria and feelings of great power. The high produced is similar to that produced by injection of high doses of amphetamines. Because cocaine is such a short-acting drug, users may continue to repeat dosages.
Hallucinations may develop with continued use, as well as violent behavior. An overdose of cocaine produces tremors, convulsions, and delirium. Death may result from a cardiovascular collapse or respiratory failure.
Cocaine users may have dilated pupils, high levels of energy and activity, and excited speech.
Dependence on amphetamines
Some psychological dependence occurs with the continued use of amphetamines. Previously, these drugs were used to control weight and obesity. However, some studies have shown that their effectiveness in reducing appetite decreases after 30days of use; therefore, they have little or no place today in the treatment of overweight patients. There is significant sale of fake amphetamines. As a result, the FDA has outlawed the manufacture of fakes by declaring that any combination of a stimulant phenethylamine with caffeine is a new drug that must be registered with the agency.
Symptoms and signs
These drugs are widely used as stimulants and generally cause elevated mood, increased wakefulness, alertness, concentration, and physical performance. They may also produce a feeling of well-being.
The withdrawal syndrome, if one exists, is not severe. Withdrawal is usually followed by a state of mental and physical depression and fatigue. The psychological dependence of the drug varies. Amphetamines are different from cocaine in that they induce tolerance. This tolerance develops slowly and an ever-increasing dosage can permit the ingestion of amounts much greater than therapeutically prescribed. The tolerance to various effects is different. Nervousness and sleeplessness may occur along with hallucinations. Massive doses are rarely fatal. Abusers are prone to accidents because of their excited state and the excessive fatigue that follows usage.
Although there are no real withdrawal effects other than sleepiness and fatigue, the abrupt discontinuation of the drugs may bring on depression, often with suicide potential. Usually, reassurance and a quiet, nonthreatening environment will encourage the person to recover.
Dependence on hallucinogens
Hallucinogens include LSD, psilocybin (magic mushrooms), mescaline (made from peyote cactus), ketamine (anesthetic used on both humans and animals) and methylene dioxymethamphetamine (MDMA). In recent years, a number of samples of a street product called Ecstasy have contained relatively pure methylene dioxyamphetamine (MDA). Unfortunately, new hallucinogens are being created by amateur chemists trying to stay ahead of the laws. Even more unfortunately, they can be more powerful and dangerous than existing hallucinogens with unknown results.
Psychic dependence on hallucinogens varies greatly but usually is not intense. There is no evidence of physical dependence when the drugs are abruptly withdrawn. LSD users can develop a high degree of tolerance but it disappears quickly (3days to a week). Individuals who are tolerant to any one of these drugs are cross-tolerant to the others. The greatest dangers to the user are psychological effects and impaired judgment. Some persons, particularly those who are repeated users of the hallucinogens, especially LSD, may experience drug effects after discontinued use. These effects are commonly referred to as “flashbacks”, which usually consist of visual illusions. Flashbacks can be brought on by use of marijuana, alcohol, or barbiturates; by stress or fatigue; or they may occur without apparent reason. What produces flashbacks is not known, but they tend to decrease in frequency over a period of 6months to one year.
Symptoms and signs
These substances induce a state of excitation and mood change from euphoric to depressive. Physical signs of usage may include dilated pupils, dry mouth, sweating or chills, blurred vision, weakness, rapid heart rate, nausea, dizziness, and an inability to perform complex tasks, such as driving or operating machinery.
Dependence on phencyclidine
Phencyclidine (PCP, also known as angel dust) has emerged as an important drug of abuse. It is not easily classified and should be considered separately from the hallucinogenic drugs. PCP was tested as an anesthetic agent in humans in the late 1950s. It was withdrawn because people experienced severe anxiety and delusions. Clinical testing stopped in 1962 and PCP appeared as a street drug in 1967. Initially sold as THC, in recent years, it has established its own market. Occasionally injected or ingested, it is most frequently sprinkled on smoking material and inhaled. Since the frequent reports of problems with PCP in 1978, the number of reports has declined significantly.
Symptoms and signs
PCP causes a wide range of effects. A giddy euphoria usually occurs with low doses, often followed by bursts of anxiety. Effects of higher doses include a withdrawn catatonic state. In treatment, diazepam (valium) is often helpful. Physical signs of usage include dilated (large) pupils, slurred speech, blank stare, rapid eye movements, strange or uncoordinated gait, lack of pain response, high blood pressure, and rapid heartbeat.
Prescription drugs
Prescription drug abuse is a rapidly growing problem in this country. In September 2013, an article by the National Institutes of Health estimated that 20% of the people in the United States have used prescription drugs for nonmedical reasons.
Prescription drugs are much more readily available than illegal drugs. Everyone probably knows someone who has unused medication in their home. Patients can go from doctor to doctor obtaining prescriptions from each one, and some unscrupulous doctors function as little more than pill dispensers. Prescription drugs can be also be obtained over the internet, sometimes without prescription or identification.
The most commonly abused prescription medications include the following:
• OxyContin, Percocet, Vicodin, Fentanyl, Methadone, and Codeine (all opioids used to treat pain).
• Xanax, Valium, and Ativan (all depressants used to treat anxiety).
• Adderall, Ritalin, and Concerta (all amphetamine-like drugs to treat ADHD).
Used in the prescribed manner, these drugs are unlikely to cause addiction. However, when they are used incorrectly over an extended period of time, tolerance, dependency, and addiction can develop quickly.
When a tablet is crushed and then swallowed, snorted, or diluted in water and injected, the time-release mechanism is destroyed and the user gets the full effects immediately. For example, some have said the effect of OxyContin used in this way is similar to heroin.
Some over-the-counter (OTC) drugs are also used in large, potentially dangerous doses to produce a high. The most commonly misused OTC drugs are cough and cold remedies containing dextromethorphan.
Symptoms and signs
These substances produce the same effects as their illegal drug counterparts: dizziness, dilated pupils, slurred words, etc.
For the security officer, it is immaterial if an employee is using illegal drugs, misusing prescription drugs, or abusing alcohol. The focus remains the same. He or she must be vigilant in their observations of employees displaying signs of intoxication and take the proper steps to notify the appropriate supervisor.
Security professionals must be on guard so that they do not fall victim to misusing prescription or OTC drugs themselves. Sometimes, security officers are called upon to work long hours due to call-offs by other officers, weather emergencies, fires, pipeline breakages, or any other type of emergency. The true security professional must not resort to any type of drug usage to fulfill their duties.
Indicators of drug abuse
Individuals, while at work, may continue their drug dependency and/or habit. Signs at the workplace that may indicate drug abuse include the following:
• Frequent absence or tardiness
• Unexplained absences from work during normal working hours
• Frequent telephone calls
• Frequent and lengthy visits to washrooms, locker rooms, or the parking lot
• Frequent non-work-related visits by strangers or employees from other areas
• A change in the disposition of the employee
• Frequent mood changes
• Poor appetite and weight loss
• Bloodshot eyes, runny nose, irritation in eyes
• Unusual pupil size (i.e., very contracted or dilated in all types of light)
• Wearing of long-sleeved shirts in warm weather
The role of security in addressing the problem of alcohol and drug abuse in the workplace should remain consistent and similar to other policies and procedures. Security personnel are best suited to provide information, gather intelligence, and conduct observation concerning alcohol and/or drug use on company property. In particular, security officers who are stationed at or near parking lots can provide a significant amount of information concerning:
• Employee trips to their vehicles
• Nonemployees visiting the facility
• Use of pay phones by employees
• Parking lot activities before and after work
• Condition of employees reporting to work
• Evidence of drinking (empty cans and bottles)
Additionally, employee informants may often confide in a security officer if they know their identity will remain anonymous. Any information received by a security officer either through his or her own observations or from an informant must be treated confidentially and sensitively. Speculation, rumor, and innuendo are often stated as fact so as to embarrass or discredit an employee or the security officer reporting the information. Security personnel should always document reports of drug or alcohol activity at the workplace and report the same to their supervisor. Security personnel may be asked to serve as a witness for a supervisor who suspects an employee may be engaged in drug or alcohol use on company property.
It should be the responsibility of the security department to properly recover, record, identify, secure, and store the evidence of suspected alcohol or drug activity. Plastic, self-sealing envelopes can often be purchased from a local supplier or law enforcement agency.
Security can provide a valuable service, in conjunction with the human resources department, by providing and/or coordinating the training of all supervisors and security personnel about drug awareness and the procedures that are to be followed when an employee is suspected of drug or alcohol use at work. Local law enforcement agencies are usually an excellent resource in providing some basic training and indoctrination of drug awareness to management personnel. These presentations will often allow the participants to view firsthand what a particular drug looks like and smells like when used. Educating the entire workforce to the problems associated with alcohol and drug abuse is a key role that security can provide for any organization.
Often, to accurately detect whether or not a drug problem exists within an organization, undercover investigators are employed to obtain and gather information. Security officers would normally never be informed that an undercover investigator is being used. Naturally, if a security officer would suspect that a person is an undercover investigator, this suspicion should never be discussed with anyone for fear of endangering the person’s safety.
Security personnel should be primarily concerned with alcohol and drug abuse by employees at the workplace. Security personnel are best suited to provide information, gather intelligence, and conduct observation concerning alcohol and/or drug abuse on company property. Any information received by a security officer concerning possible alcohol or drug-related activity at work should never be discussed with anyone other than the officer’s immediate supervisor.
Summary
• A single definition for drug dependence is impossible. Addiction refers to a style of living that includes drug dependence. Dependence can be physical and/or psychological.
• Required by law, The Comprehensive Drug Abuse and Prevention Act of 1970 divides controlled substances into five classes or schedules. Those in Schedule I have the highest potential for abuse with no accepted medical use. Prescriptions for drugs in all these schedules must show the physician’s FDA license number.
• Alcoholism is a chronic illness that costs the U.S. economy $223.5billion dollars a year. It is estimated 67% of Americans drink alcoholic beverages and that one in six will experience some problem with alcoholism.
• Since 1909, the federal government has attempted to control opium use. Opioid type drugs are considered narcotic and are effective as pain relievers. Opioid drugs include opium, morphine, heroin, codeine, and methadone.
• Other drugs that may be abused include: barbiturates, marijuana, cocaine, amphetamines, PCP, hallucinogens, and prescription drugs. Amateur chemists, in the attempt to stay ahead of the laws, are continually creating new formulas for old drugs as well as creating new ones.
• An ever-growing problem in this country is prescription drug abuse. The most commonly abused drugs include OxyContin, Percocet, Vicodin, Fentanyl, Methadone, Codeine, Xanax, Valium, Ativan, Adderall, Ritalin, and Concerta.
• Some symptoms and signs of alcohol or drug use include dilated pupils, bloodshot eyes, runny nose, dizziness, sweating or chills, nausea, slurred or excited speech, anxiety or paranoia, increased heart rate and blood pressure, and an inability to perform complex tasks, such as driving or operating machinery.
• Indicators of drug abuse in the workplace also may include frequent tardiness or absence; telephone calls; lengthy visits to washrooms, locker rooms, or the parking lots; mood changes; and non-work-related visits by strangers or employees from other areas. A change in the disposition of an employee, extreme weight loss, and the wearing of long-sleeved shirts in warm weather also may be signs of a drug habit.
• Security personnel are best suited to provide information, gather intelligence, and conduct observation concerning alcohol and/or drug use on company property.
• Any information received by a security officer must be kept confidential. Any reports of drug or alcohol activity at the workplace should be documented and reported to the supervisor.
• It should be the responsibility of the security department to properly recover, record, identify, secure, and store the evidence of suspected alcohol or drug activity.
Exercises
1. What is drug abuse?
2. What is the Comprehensive Drug Abuse and Prevention Act of 1970?
3. What is alcoholism?
4. What are indicators of alcohol or drug abuse?
5. What is the role of security personnel in addressing the problem of alcohol and drug abuse in the workplace?
Blood alcohol concentration (%BAC) guide
The measure of impairment is directly related to several factor such as weight, gender, and body metabolism. Women are more susceptible to the effects of alcohol than men. The following charts are organized based on weight and gender only.